Korean J Urol.
2012 Mar;53(3):154-158.
Effects of Partial Nephrectomy on Postoperative Blood Pressure
- Affiliations
-
- 1Ludwig Institute for Cancer Research, Department of Surgery, Austin Hospital, University of Melbourne Faculty of Medicine, Heidelberg, Australia. lawrentschuk@gmail.com
- 2Department of Surgical Oncology, University of Toronto, Toronto, Canada.
- 3Department of Urology, Dalhousie University Faculty of Medicine, Halifax, Canada.
Abstract
- PURPOSE
The effects of partial nephrectomy (PN) on postoperative blood pressure (BP) are not known, and PN has the potential to worsen BP. We therefore sought to determine whether PN alters postoperative BP.
MATERIALS AND METHODS
Patients who underwent PN for suspected malignancy at our institution from 2002 to 2008 were included. Data on BP and medication from before and after PN were retrieved from family physicians. BP and number of antihypertensive medications were compared after surgery with preoperative values by use of paired t tests and Chi-squared analyses, respectively.
RESULTS
Of 74 patients undergoing PN and providing consent, 48 met the inclusion and exclusion criteria, with a median follow-up of 24 months. For the early postoperative period (1 month to 1 year after surgery), the mean BPs (132.3/77.0 mmHg) were unchanged compared with preoperative values (132.4/78.0 mmHg; p=0.59 systolic BP and p=0.30 diastolic BP). For the later postoperative period (beyond 1 year after surgery), the mean postoperative systolic BP was unchanged from the mean preoperative systolic BP (131.2 mmHg vs. 132.4 mmHg, respectively; p>0.30). However, the corresponding average diastolic BP was lower in the long term (78.0 mmHg versus 76.4 mmHg respectively; p=0.01). No significant difference in the mean number of BP medications prescribed preoperatively, at one year, and beyond one year was identified (p>0.37).
CONCLUSIONS
PN does not result in initial or long-term postoperative deterioration in BP.
MeSH Terms
Figure
-
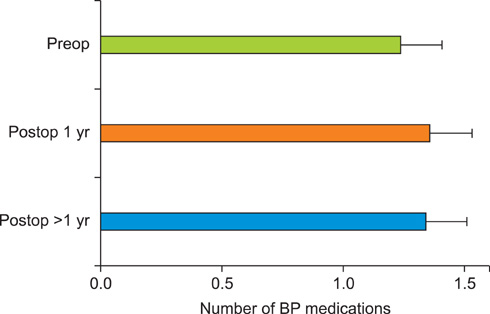
FIG. 1 Mean number of medications taken per patient before surgery compared with at 1 year after surgery and beyond 1 year at the last follow-up (p>0.37).
Reference
-
1. Gill IS, Aron M, Gervais DA, et al. Clinical practice. Small renal mass. N Engl J Med. 362:624–634.2. Uzzo RG, Novick AC. Nephron sparing surgery for renal tumors: indications, techniques and outcomes. J Urol. 2001. 166:6–18.3. Lau WK, Blute ML, Weaver AL, et al. Matched comparison of radical nephrectomy vs nephron-sparing surgery in patients with unilateral renal cell carcinoma and a normal contralateral kidney. Mayo Clin Proc. 2000. 75:1236–1242.4. Dash A, Vickers AJ, Schachter LR, et al. Comparison of outcomes in elective partial vs radical nephrectomy for clear cell renal cell carcinoma of 4-7 cm. BJU Int. 2006. 97:939–945.5. Weight CJ, Larson BT, Fergany AF, et al. Nephrectomy induced chronic renal insufficiency is associated with increased risk of cardiovascular death and death from any cause in patients with localized cT1b renal masses. J Urol. 2010. 183:1317–1323.6. Huang WC, Elkin EB, Levey AS, et al. Partial nephrectomy versus radical nephrectomy in patients with small renal tumors--is there a difference in mortality and cardiovascular outcomes? J Urol. 2009. 181:55–61.7. Malcolm JB, Bagrodia A, Derweesh IH, et al. Comparison of rates and risk factors for developing chronic renal insufficiency, proteinuria and metabolic acidosis after radical or partial nephrectomy. BJU Int. 2009. 104:476–481.8. Zorn KC, Gong EM, Orvieto MA, et al. Comparison of laparoscopic radical and partial nephrectomy: effects on long-term serum creatinine. Urology. 2007. 69:1035–1040.9. Johns C, Gavras I, Handy DE, et al. Models of experimental hypertension in mice. Hypertension. 1996. 28:1064–1069.10. Ploth DW, Fitzgibbon W. Pathophysiology of altered renal function in renal vascular hypertension. Am J Kidney Dis. 1994. 24:652–659.11. Uchida K, Takahashi A, Masumori N, et al. Partial nephrectomy for small localized renal cell carcinoma. Hinyokika Kiyo. 2004. 50:389–395.12. Goel RK, Hickey LT, Rendon RA. Malignant hypertension due to renal artery stenosis after open partial nephrectomy in a solitary kidney. Urology. 2007. 69:385.e5–385.e7.13. John J, Allen S, Perry M, et al. Page kidney phenomenon presenting as acute renal failure after partial nephrectomy: a case report and review of the literature. Urol Int. 2008. 80:440–443.14. Novick AC, Gephardt G, Guz B, et al. Long-term follow-up after partial removal of a solitary kidney. N Engl J Med. 1991. 325:1058–1062.15. Moudouni SM, Hadj Slimen M, Manunta A, et al. Management of major blunt renal lacerations: is a nonoperative approach indicated? Eur Urol. 2001. 40:409–414.16. Nicol AJ, Theunissen D. Renal salvage in penetrating kidney injuries: a prospective analysis. J Trauma. 2002. 53:351–353.17. Al-Qudah HS, Santucci RA. Complications of renal trauma. Urol Clin North Am. 2006. 33:41–53. vi18. Azar SA, Nakhjavani MR, Tarzamni MK, et al. Is living kidney donation really safe? Transplant Proc. 2007. 39:822–823.19. Fehrman-Ekholm I. Living donor kidney transplantation. Transplant Proc. 2006. 38:2637–2641.20. Najarian JS, Chavers BM, McHugh LE, et al. 20 years or more of follow-up of living kidney donors. Lancet. 1992. 340:807–810.21. Stojanovic M, Goldner B, Ivkovic D. Renal cell carcinoma and arterial hypertension. Clin Exp Nephrol. 2009. 13:295–299.22. Onysko J, Maxwell C, Eliasziw M, et al. Large increases in hypertension diagnosis and treatment in Canada after a healthcare professional education program. Hypertension. 2006. 48:853–860.23. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC Cancer Staging Manual. 2010. 7th ed. New York: Springer.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Partial Nephrectomy Using in Situ Hypothermia
- Current Status of Partial Nephrectomy for Renal Mass
- 2 Cases of Consecutive Partial Nephrectomy after Nephrolithotomy in Renal Stone
- Non-ischemic Partial Nephrectomy with Using the Microwave Tissue Coagulator
- Laparoscopic Partial Nephrectomy using a Microwave Tissue Coagulator for Small Renal Tumor
