Usefulness of DeltaFEV0.75 and DeltaFEV0.5 for Airway Reversibility in Preschoolers with Asthma
- Affiliations
-
- 1Department of Pediatrics, Institute of Allergy, Yonsei University College of Medicine, Seoul, Korea. mhsohn@yuns.ac
Abstract
- PURPOSE
Preschoolers complete forced expiration in a short time, sometimes more quickly than in 1 second, and therefore the importance of forced expiatory volume in 0.75 seconds (FEV0.75) or forced expiatory volume in 0.5 seconds (FEV0.5) has been raised. The purpose of this study is to evaluate the clinical usefulness of DeltaFEV0.75 and DeltaFEV0.5.
METHODS
We analyzed 401 subjects of an asthma group, and 150 subjects of a control group under 7 years of age.
RESULTS
DeltaFEV1, DeltaFEV0.75 and DeltaFEV0.5 values of the asthma group were significantly higher than those of the control group, respectively (P<0.0001). DeltaFEV1 (0.60; 95% confidence interval [CI], 0.57 to 0.62), DeltaFEV0.75 (0.61; 0.58 to 0.65), and DeltaFEV0.5 (0.60; 0.56 to 0.64) showed no significant difference in the diagnostic ability of asthma when airway reversibility is defined as DeltaFEVt> or =12%. Cutoff values for asthma were 8.6% in DeltaFEV1, 7.9% in DeltaFEV0.75 and 14.2% in DeltaFEV0.5. DeltaFEV0.75 (0.91; 0.88 to 0.94) showed significantly higher area under curve (AUC) than DeltaFEV0.5 (0.77; 0.73 to 0.82) when stratified by 12%, in predicting airway reversibility defined as DeltaFEV1> or =12%. Cutoff values were 12.3% in DeltaFEV0.75, and 13.4% in DeltaFEV0.5. When airway reversibility is defined as DeltaFEV1> or =8.6%, DeltaFEV0.75 (0.90; 0.87 to 0.92) also showed significantly higher AUC than DeltaFEV0.5 (0.79; 0.75 to 0.82), and Cutoff values were 8.4% in DeltaFEV0.75, and 11.3% in DeltaFEV0.5.
CONCLUSION
DeltaFEV0.75 or DeltaFEV0.5 can be a means to replace DeltaFEV1 for diagnosis of asthma and assessment of airway reversibility in preschool children.
Figure
-

Fig. 1 Receiver operating characteristic (ROC) curves of ΔFEV1, ΔFEV0.75 and ΔFEV0.5 for diagnosis of asthma when bronchodilator response is defined as ΔFEVt≥12%. ΔFEV1 (0.60; 95% confidence interval, 0.57-0.62), ΔFEV0.75 (0.61, 0.58-0.65), and ΔFEV0.5 (0.60, 0.56-0.64) showed no significant difference in area under curve of ROC curves. FEV1, forced expiratory volume in 1 second; FEV0.75, forced expiratory volume in 0.75 second; FEV0.5, forced expiratory volume in 0.5 second.
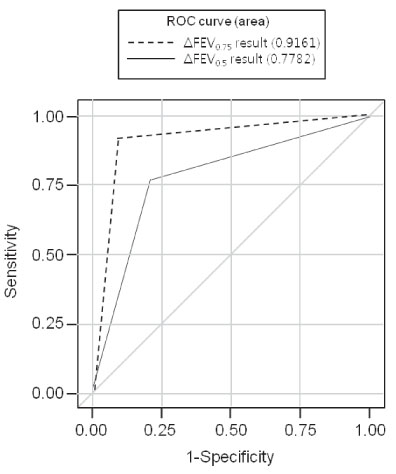
Fig. 2 Receiver operating characteristic (ROC) curves ΔFEV0.75 and ΔFEV0.5 when stratified by 12% for airway reversibility defined as ΔFEV1≥12%. ΔFEV0.75 (0.91, 0.88-0.94) showed significantly higher area under curve than ΔFEV0.5 (0.77, 0.73-0.82). FEV0.75, forced expiratory volume in 0.75 second; FEV0.5, forced expiratory volume in 0.5 second.

Fig. 3 Receiver operating characteristic (ROC) curves ΔFEV0.75 and ΔFEV0.5 when stratified by 8.6% for airway reversibility defined as ΔFEV1≥8.6%. ΔFEV0.75 (0.90, 0.87-0.92) showed significantly higher area under curve than ΔFEV0.5 (0.79, 0.75-0.82). FEV0.75, forced expiratory volume in 0.75 second; FEV0.5, forced expiratory volume in 0.5 second.
Reference
-
1. National Institutes of Health, National Heart, Lung, and Blood Institute. Global initiative for asthma. Global strategy for asthma management and prevention. 2010. Bethesda: National Institutes of Health, National Heart, Lung, and Blood Institute;18.2. American Thoracic Society. Standardization of Spirometry, 1994 Update. Am J Respir Crit Care Med. 1995. 152:1107–1136.3. Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC. Lung volumes and forced ventilatory flows. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur Respir J Suppl. 1993. 16:5–40.4. National Institutes of Health, National Heart, Lung, and Blood Institute. Expert Panel Report 2. Guidelines for the diagnosis and management of asthma. 1997. Bethesda: National Institutes of Health, National Heart, Lung, and Blood Institute;17–19.5. American Thoracic Society. Lung function testing: selection of reference values and interpretative strategies. Am Rev Respir Dis. 1991. 144:1202–1218.6. Kanengiser S, Dozor AJ. Forced expiratory maneuvers in children aged 3 to 5 years. Pediatr Pulmonol. 1994. 18:144–149.
Article7. Merkus PJ, Mijnsbergen JY, Hop WC, de Jongste JC. Interrupter resistance in preschool children: measurement characteristics and reference values. Am J Respir Crit Care Med. 2001. 163:1350–1355.8. Vilozni D, Barak A, Efrati O, Augarten A, Springer C, Yahav Y, et al. The role of computer games in measuring spirometry in healthy and "asthmatic" preschool children. Chest. 2005. 128:1146–1155.
Article9. Aurora P, Stocks J, Oliver C, Saunders C, Castle R, Chaziparasidis G, et al. Quality control for spirometry in preschool children with and without lung disease. Am J Respir Crit Care Med. 2004. 169:1152–1159.
Article10. Seo HK, Chang SJ, Jung DW, Wee YS, Jee HM, Seo JY, et al. The quality control and acceptability of spirometry in preschool children. Korean J Pediatr. 2009. 52:1267–1272.
Article11. Nève V, Edme JL, Devos P, Deschildre A, Thumerelle C, Santos C, et al. Spirometry in 3-5-year-old children with asthma. Pediatr Pulmonol. 2006. 41:735–743.
Article12. Eigen H, Bieler H, Grant D, Christoph K, Terrill D, Heilman DK, et al. Spirometric pulmonary function in healthy preschool children. Am J Respir Crit Care Med. 2001. 163(3 Pt 1):619–623.
Article13. Nystad W, Samuelsen SO, Nafstad P, Edvardsen E, Stensrud T, Jaakkola JJ. Feasibility of measuring lung function in preschool children. Thorax. 2002. 57:1021–1027.
Article14. Vilozni D, Barker M, Jellouschek H, Heimann G, Blau H. An interactive computer-animated system (SpiroGame) facilitates spirometry in preschool children. Am J Respir Crit Care Med. 2001. 164:2200–2205.
Article15. Jones MH, Davis SD, Grant D, Christoph K, Kisling J, Tepper RS. Forced expiratory maneuvers in very young children. Assessment of flow limitation. Am J Respir Crit Care Med. 1999. 159:791–795.16. Zapletal A, Chalupová J. Forced expiratory parameters in healthy preschool children (3-6 years of age). Pediatr Pulmonol. 2003. 35:200–207.
Article17. Marostica PJ, Weist AD, Eigen H, Angelicchio C, Christoph K, Savage J, et al. Spirometry in 3- to 6-year-old children with cystic fibrosis. Am J Respir Crit Care Med. 2002. 166:67–71.
Article18. Crenesse D, Berlioz M, Bourrier T, Albertini M. Spirometry in children aged 3 to 5 years: reliability of forced expiratory maneuvers. Pediatr Pulmonol. 2001. 32:56–61.
Article19. Gracchi V, Boel M, van der Laag J, van der Ent CK. Spirometry in young children: should computer-animation programs be used during testing? Eur Respir J. 2003. 21:872–875.
Article20. Kozlowska W, Aurora P, Stocks J. The use of computer-animation programs during spirometry in preschool children. Eur Respir J. 2004. 23:494–495.
Article21. Pesant C, Santschi M, Praud JP, Geoffroy M, Niyonsenga T, Vlachos-Mayer H. Spirometric pulmonary function in 3- to 5-year-old children. Pediatr Pulmonol. 2007. 42:263–271.
Article22. Piccioni P, Borraccino A, Forneris MP, Migliore E, Carena C, Bignamini E, et al. Reference values of forced expiratory volumes and pulmonary flows in 3-6 year children: a cross- sectional study. Respir Res. 2007. 8:14.23. Beydon N, Davis SD, Lombardi E, Allen JL, Arets HG, Aurora P, et al. An official American Thoracic Society/European Respiratory Society statement: pulmonary function testing in preschool children. Am J Respir Crit Care Med. 2007. 175:1304–1345.
Article24. Malmberg LP, Pelkonen A, Koljonen P, Syva-Ènen P, Nikander K, Haahtela T, et al. Assessing changes in airway obstruction during challenge tests in child asthmatics-which spirometric indices? Eur Respir J (Suppl). 1999. 14:12.25. Lim DH, Kim JH, Son BK, Rha YH. Spirometric pulmonary function test in preschool children. J Korean Med Assoc. 2010. 53:417–423.
Article26. Song TW, Kim KW, Kim ES, Park JW, Sohn MH, Kim KE. Utility of impulse oscillometry in young children with asthma. Pediatr Allergy Immunol. 2008. 19:763–768.
Article27. Lee JH, Choi BS, Baek JY, Lee YJ, Kim KW, Sohn MH, et al. Comparison of exhaled nitric oxide analyzers in childhood asthma. Pediatr Allergy Respir Dis. 2011. 21:17–23.
Article28. Baek JY, Choi BS, Lee YJ, Park YH, Kim KW, Sohn MH, et al. Clinical implication of sputum CXCL13 in children with asthma. Pediatr Allergy Respir Dis. 2009. 19:420–428.
Article29. Chernick V, Boat TF, Wilmott RW, Bush A. Kendig's disorders of the respiratory tract in children. 2006. 7th ed. Philadelphia: Saunders Elsevier.30. Suh DI, Lee JK, Lee JH, Koh YY. Bronchodilator response and its relationship to bronchial hyperresponsiveness in children with allergic rhinitis/asthma. Pediatr Allergy Respir Dis. 2010. 20:59–67.31. Dales RE, Spitzer WO, Tousignant P, Schechter M, Suissa S. Clinical interpretation of airway response to a bronchodilator. Epidemiologic considerations. Am Rev Respir Dis. 1988. 138:317–320.
Article32. Strachan DP. Repeatability of ventilatory function measurements in a population survey of 7 year old children. Thorax. 1989. 44:474–479.
Article33. Dundas I, Chan EY, Bridge PD, McKenzie SA. Diagnostic accuracy of bronchodilator responsiveness in wheezy children. Thorax. 2005. 60:13–16.
Article34. Galant SP, Morphew T, Amaro S, Liao O. Value of the bronchodilator response in assessing controller naïve asthmatic children. J Pediatr. 2007. 151:457–462. 462.e1
Article35. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982. 143:29–36.
Article36. Warwick WJ. Pulmonary function in healthy Minnesota children. Minn Med. 1977. 60:435–440.37. Chipps BE. Asthma in infants and children. Clin Cornerstone. 2008. 8:44–61.
Article38. Castro-Rodríguez JA, Holberg CJ, Wright AL, Martinez FD. A clinical index to define risk of asthma in young children with recurrent wheezing. Am J Respir Crit Care Med. 2000. 162(4 Pt 1):1403–1406.
Article39. Beydon N. Pulmonary function testing in young children. Paediatr Respir Rev. 2009. 10:208–213.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Usefulness of Impulse Oscillometry in Estimation of the Reversibility of Airway Obstruction in Adult Asthmatics
- Role of Bronchodilator Reversibility Testing in Differentiating Asthma From COPD
- Evolution of Asthma Concept and Effect of Current Asthma Management Guidelines
- Current Trends in Asthma
- The Complementary Role of FEV6 in Bronchodilator Reversibility Test for the Old Age
