Korean J Urol.
2010 May;51(5):362-364.
Calculi in Hydrocele: Incidence and Results of Infrared Spectroscopy Analysis
- Affiliations
-
- 1Department of Urology Oncology Nephrology, Klinik Wildetal, Bad Wildungen-Reinhardshausen, Germany. Winfried.Vahlensieck@t-online.de
- 2Department of Urology, University of Bonn, Germany.
Abstract
- Trauma, inflammation, or necrosis in the scrotal cavity may lead to depositing of organic material in hydrocele fluid with consecutive calcification if the fluid is oversaturated. During a period of 25 years, 2 scrotal calculi (calculous material in hydrocele fluid) in 2 of 42 patients (4.8%) were found during surgery on symptomatic hydroceles by the first author. In these symptomatic cases, infrared spectroscopy revealed carbonate apatite as the causative mineral. The appearance of scrotal calculi in hydrocele does not change the treatment or prognosis of hydroceles. However, if the calculous material is attached to the visceral or parietal part of the tunica vaginalis and does not change position during sonography with different postures, tumor growth may be a problem. An inguinal approach for operation should be chosen in such situations. Infrared spectroscopy can be used to determine the mineralogy of scrotal calculi. Carbonate apatite, the predominantly found mineral in scrotal calculi, can precipitate in an alkaline milieu.
MeSH Terms
Figure
-
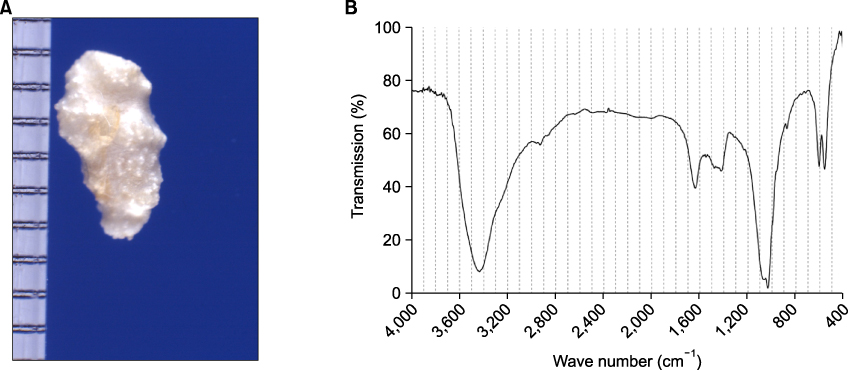
FIG. 1 (A) A 2 g rough, white scrotal calculus. (B) Infrared spectroscopy of the stone in (A) showing 100% carbonate apatite.

FIG. 2 An 11 g, bizarre-shaped, brown scrotal calculus.
Reference
-
1. Hesse A, Sanders G. Atlas of infrared spectra for the analysis of urinary concrements. 1988. 1st ed. Stuttgart New York: Thieme;37.2. Chatterjee AC. A rare complication of hydrocele. Br J Surg. 1975. 62:891–892.3. Gakiya M, Nakai H, Higuchi A, Shishido S, Kawamura T. Scrotal calcification associated with hydrocele testis in a child: a case report. Hinyokika Kiyo. 1994. 40:845–847.4. Török P, Perjés G, Rosdy E. Intrascrotal calcification. Int Urol Nephrol. 1981. 13:167–173.5. Hussein O, El Setouhy M, Ahmed ES, Kandil AM, Ramzy RM, Helmy H, et al. Duplex Doppler sonographic assessment of the effects of diethylcarbamazine and albendazole therapy on adult filarial worms and adjacent host tissues in Bancroftian filariasis. Am J Trop Med Hyg. 2004. 71:471–477.6. Frauscher F, Klauser A, Stenzl A, Helweg G, Amort B, zur Nedden D. US findings in the scrotum of extreme mountain bikers. Radiology. 2001. 219:427–431.7. Sánchez Merino JM, Lancina Martín A, Grases Freixedas F, Parra Muntaner L, Gómez Cisneros SC, García Alonso J. Intra-scrotal lithiasis. Crystallographic analysis. Arch Esp Urol. 2002. 55:523–526.8. Namjoshi SP. Calculi in hydroceles: sonographic diagnosis and significance. J Clin Ultrasound. 1997. 25:437–441.9. Martin B, Tubiana JM. Significance of scrotal calcifications detected by sonography. J Clin Ultrasound. 1988. 16:545–552.10. Sugishita K, Kashiwagi A, Nagamori S, Yamashiro K, Sato N. Serous papillary adenocarcinoma of the tunica vaginalis of the testis: a case report. Nippon Hinyokika Gakkai Zasshi. 2004. 95:626–629.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Infrared Spectroscopy Analysis of the Urinary Calculi of Korean People
- Infrared Spectroscopy Analysis of Urinary Calculi
- Analysis of the Urinary Calculi by Infrared Spectroscopy
- Clinical Application of Near Infrared Spectroscopy
- Identification and quantification of intrahepatic calculi by infrared absorption spectroscopy
