Robot-Assisted Laparoscopic Radical Prostatectomy
- Affiliations
-
- 1Department of Urology, Urological Science Institute, Yonsei University College of Medicine, Seoul, Korea. khrha@yuhs.ac
Abstract
- PURPOSE
Laparoscopic radical prostatectomy is an alternative to open prostatectomy in the surgical management of prostate cancer. The introduction of surgical robot to assist laparoscopic surgery served as a mechanical device to enhance the laparoscopic skills and improve surgical maneuverability with enhanced visual systems and the multi-axis articulating instruments. This review will introduce the evolution of surgical technique and current status of robotic-assisted laparoscopic prostatectomy.
MATERIALS AND METHODS
A review of literatures is conducted with the homepage of Korean Urologic Association and PubMed, a search tool of the National Library of Medicine and the National Institutes of Health, including the MEDLINE database.
RESULTS
After its approval by the United States FDA in 2000, the robotic technology has revolutionized the treatment of surgical management of prostate cancer. Robotic-assisted laparoscopic radical prostatectomy offers benefits of minimally invasive surgery with comparable oncological functional outcomes compared to standard surgical options.
CONCLUSIONS
This technique is expected to evolve into one of the standard of care in treatment of localized prostate cancer.
Keyword
MeSH Terms
Figure
-
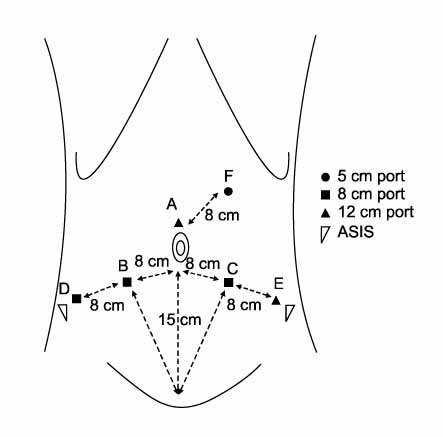
Fig. 1 Trocar placement for the transperitoneal approach. The letters represent the sequence of trocar placement. (A) Supraumbilical 12 mm camera port. (B, C) Eight mm ports for the robot instruments placed 8 cm laterocaudal to the camera port and 15 cm cranial to the pubis symphysis. (D) Eight mm ports for the 4th arm placed 8 cm laterocaudal to the B port in a direction toward the anterior superior iliac spine (ASIS). (E) Twelve mm port for an assistant instrument placed 8 cm laterocaudal to the C port in a direction toward the ASIS. (F) Five mm port for assistant's suction placed approximately 8 cm cranial to the midline of the A and C ports.
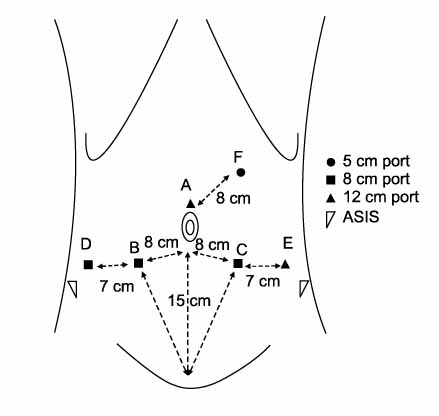
Fig. 2 Trocar placement for a small pelvis. The letters represent the sequence of trocar placement. (A) Supraumbilical 12 mm camera port. (B, C) Eight mm ports for the robot instruments placed 8 cm laterocaudal to the camera port and 15 cm cranial to the pubis symphysis. (D) Eight mm ports for the 4th arm placed 7 cm horizontal to the B port to avoid the anterior superior iliac spine (ASIS). (E) Twelve mm port for an assistant instrument placed 7 cm horizontal to the C port to avoid the ASIS. (F) Five mm port for assistant's suction placed approximately 8 cm cranial from the midline between the A and C ports.
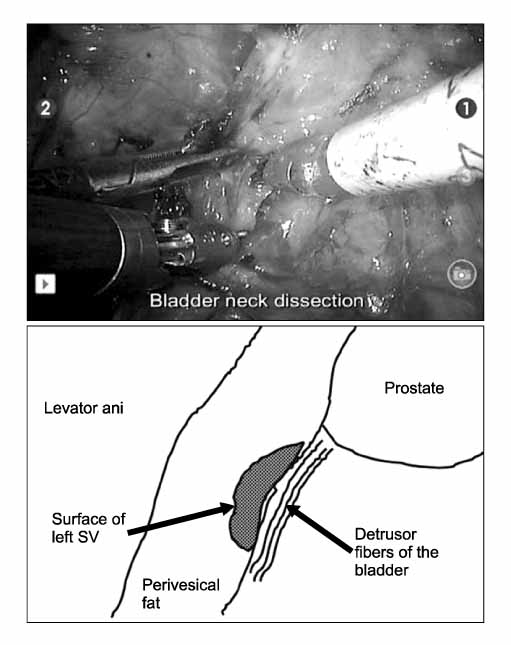
Fig. 3 Bladder neck dissection. The picture demonstrates the left-side bladder neck dissection. The detrusor muscle fibers are identified and the lateral border of the bladder neck is separated until it reaches the seminal vesicle.
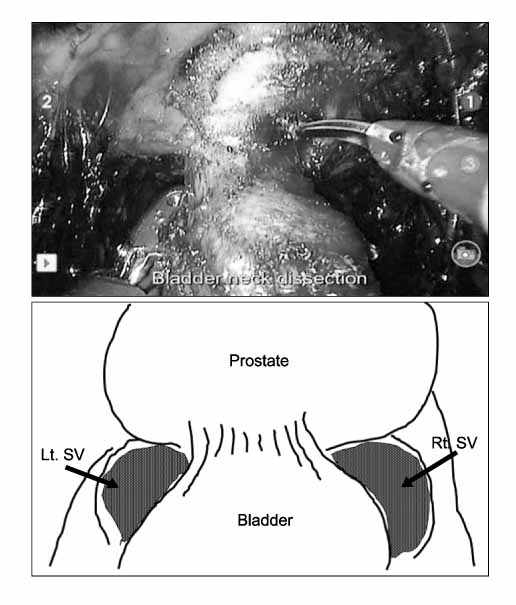
Fig. 4 Bladder neck transection. The picture demonstrates a well-preserved bladder neck. Following bilateral dissection of the bladder neck, the detrusor muscle is well appreciated. At this moment, the bladder neck is transected. This technique allows bladder neck preservation even for a prostate with a large median lobe.

Fig. 5 The da Vinci S Surgical system.
Reference
-
1. Walsh PC, Donker PJ, Lepor H, Eggleston JC. Radical prostatectomy with preservation of sexual function: Anatomical and pathological considerations. Prostate. 1983. 4:473–485.2. Schuessler WW, Kavoussi LR, Clayman RV. Laparoscopic radical prostatectomy: initial case report. J Urology. 1992. 147:246.3. Guillonneau B, Rozet F, Barret E, Cathelineau X, Vallancien G. Laparoscopic radical prostatectomy: assessment after 240 procedures. Urol Clin North Am. 2001. 28:189–202.4. Menon M, Tewari A, Peabody JO, Shrivastava A, Kaul S, Bhadari A, et al. Vattikuti Institute prostatecomy, a technique of robotic radical prostatectomy for management of localized carcinoma of the prostate: experience of over 1,100 cases. Urol Clin North Am. 2004. 31:701–717.5. Lee YS, Han WK, Oh YT, Choi YD, Yang SC, Rha KH. Robot-assisted laparoscopic radical prostatectomy: four cases. Yonsei Med J. 2007. 48:341–346.6. Park SY, Cho KS, Ham WS, Lee JH, Choi HM, Rha KH. Robot-assisted laparoscopic nephroureterectomy with a bladder cuff excision. Korean J Urol. 2008. 49:373–375.7. Park SY, Kim HJ, Seo JW, Cho KS, Ham WS, Rha KH. Robot-assisted laparoscopic partial nephrectomy. Korean J Urol. 2008. 49:387–391.8. Park SY, Cho KS, Park KK, Park SJ, Ham WS, Rha KH. Robot-assisted laparoscopic radical cystectomy with ileal conduit urinary diversion. Korean J Urol. 2008. 49:506–509.9. Curto F, Benijts J, Pansadoro A, Barmoshe S, Hoepffner JL, Mugnier C, et al. Nerve sparing laparoscopic radical prostatectomy: our technique. Eur Urol. 2006. 49:344–352.10. Capello SA, Boczko J, Patel HR, Joseph JV. Randomized comparison of extraperitoneal and transperitoneal access for robot-assisted radical prostatectomy. J Endourol. 2007. 21:1199–1202.11. Patel VR, Thaly R, Shah K. Robotic radical prostatectomy?: outcomes of 500 cases. BJU Int. 2007. 99:1109–1112.12. Patel VR, Tully AS, Holmes R, Lindsay J. Robotic radical prostatectomy in the community setting-the learning curve and beyond. Initial 200 cases. J Urol. 2005. 174:269–272.13. Menon M, Tewari A. Robotic radical prostatectomy and the Vattikuti Urology Institute technique: an interim analysis of results and technical points. Urology. 2003. 61:Suppl 4A. 15–20.15. Monon M, Shrivastava A, Kaul S, Badani KK, Fumo M, Bhandari M, et al. Vattikuti Institute Prostatectomy: comtemporary technique and analysis of results. Eur Urol. 2007. 57:648–658.16. Shah KK, Thaly R, Patel V. Early retrograde release of the neurovascular bundle during robotic radical prostatectomy. J Urol. 2007. 177:117.17. Sim HG, Yip SK, Lau WK, Tan JK, Cheng CW. Early experience with robot-assisted laparoscopic radical prostatectomy. Asian J Surg. 2004. 27:321–325.18. Rocco B, Gregori A, Stener S, Santoro L, Bozzola A, Galli S, et al. Posterior reconstruction of the rhabdosphincter allows a rapid recovery of continence after transperitoneal videolaparoscopic radical prostatectomy. Eur Urol. 2007. 51:996–1003.19. Tewari AK, Bigelow K, Rao S, Takenaka A, El-Tabi N, Te A, et al. Anatomic restoration technique of continence mechanism and preservation of puboprostatic collar: a novel modification to achieve early urinary continence in men undergoing robotic prostatectomy. Urology. 2007. 69:726–731.20. Guillonneau B, Gupta R, El Fettouh H, Cathelineau X, Baumert H, Vallancien G. Laparoscopic [correction of laproscopic] management of rectal injury during laparoscopic [correction of laproscopic] radical prostatectomy. J Urol. 2003. 169:1694–1696.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Erratum: Robot-Assisted Laparoscopic Radical Prostatectomy
- A Case of Robot-Assisted Laparoscopic Radical Prostatectomy in Primary Small Cell Prostate Cancer
- Floating Hem-o-Lok Clips in the Bladder without Stone Formation after Robot-Assisted Laparoscopic Radical Prostatectomy
- Robot-Assisted Laparoscopic Radical Prostatectomy: Four Cases
- Two Different Surgical Approaches for Prostatic Stromal Sarcoma: Robot-Assisted Laparoscopic Radical Prostatectomy and Open Radical Cysto-Prostatectomy With Ileal Conduit
