Korean J Urol.
2009 Mar;50(3):261-266.
Effects of Metabolic Syndrome on Chronic Kidney Disease
- Affiliations
-
- 1Department of Urology, Chungbuk National University College of Medicine, Cheongju, Korea. urokyj@cbnu.ac.kr
- 2Department of Urology, Konkuk University College of Medicine, Chungju, Korea.
Abstract
-
PURPOSE: Metabolic syndrome (MS) has been identified as a causal risk factor for cardiovascular disease, stroke, and cardiovascular mortality. Recent studies have suggested a possible relation between MS and renal function. The aim of this study was to evaluate the influence of MS on renal function.
MATERIALS AND METHODS
We analyzed 12,348 healthy Koreans who underwent a general health checkup. MS was defined as 3 or more of the criteria according to the National Cholesterol Education Program Adult Treatment Panel guidelines III (NCEP ATP III). The glomerular filtration rate (GFR) was estimated by the redefined Modification of Diet in Renal Disease formula. Chronic kidney disease (CKD) was categorized into 3 categories according to the Kidney Disease: Improving Global Outcomes guidelines; I: GFR> or =90 ml/min, II: 60-89 ml/min, III: 30-59 ml/min.
RESULTS
The overall proportion with MS was 19.3%. Compared with populations without MS, those with MS showed a significantly decreased GFR. The prevalence of CKD increased with the number of MS components, and it was prominent in the group of males over 40 years of age. In multivariate analyses using age, sex, and individual MS components, age (odds ratio [OR]=20.40; 95% CI: 10.81-38.49), sex (OR=1.98; 95% CI: 1.51-2.60), and obesity (OR=1.48; 95% CI: 1.13-1.93) were strongly associated with CKD.
CONCLUSIONS
This study showed that MS is a significant determinant of CKD. Handling of correctable factors such as obesity may be considered one of the preventive modalities against the development of CKD.
MeSH Terms
Figure
-
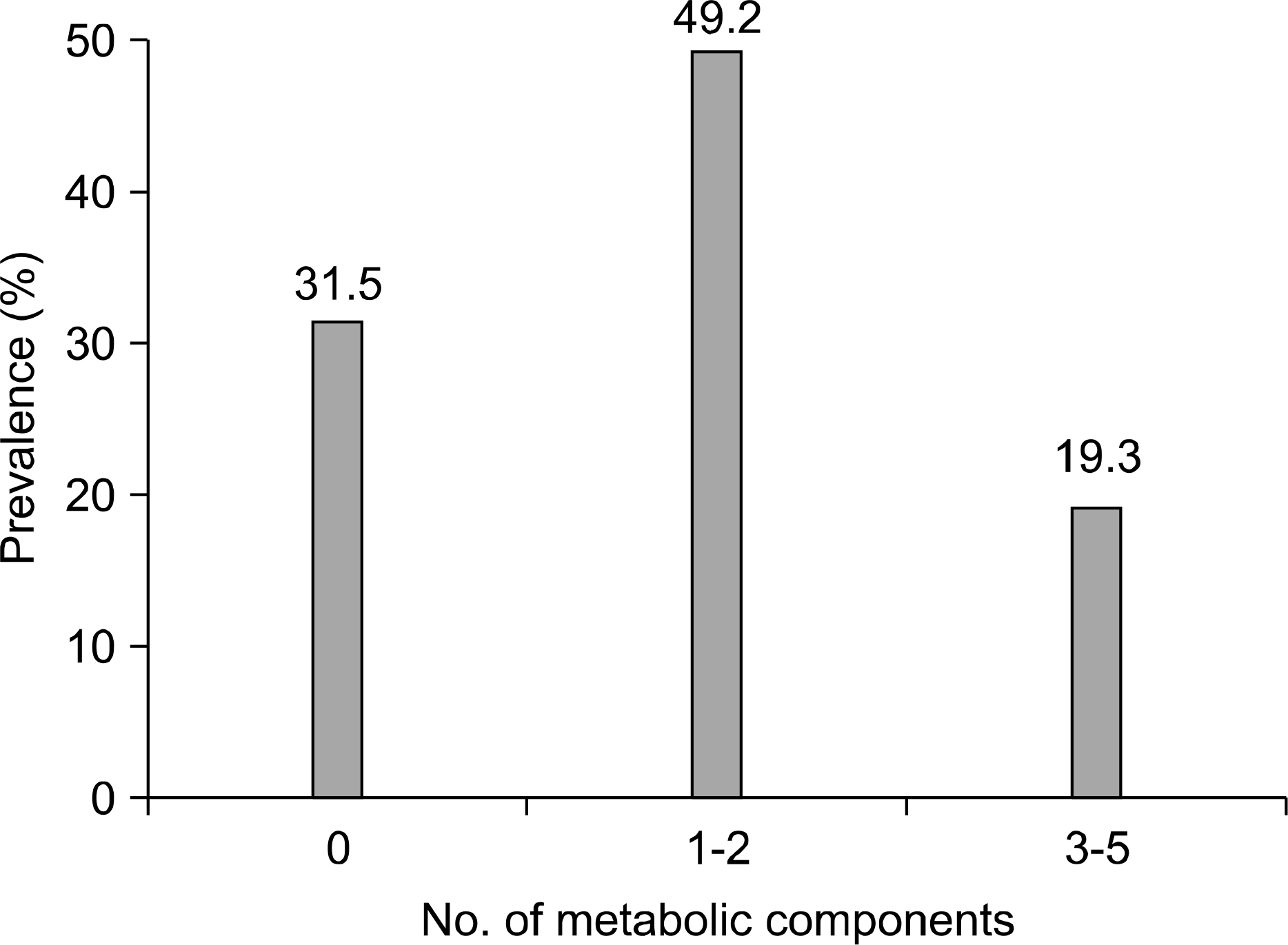
Fig. 1. The prevalence of metabolic syndrome by number of components.
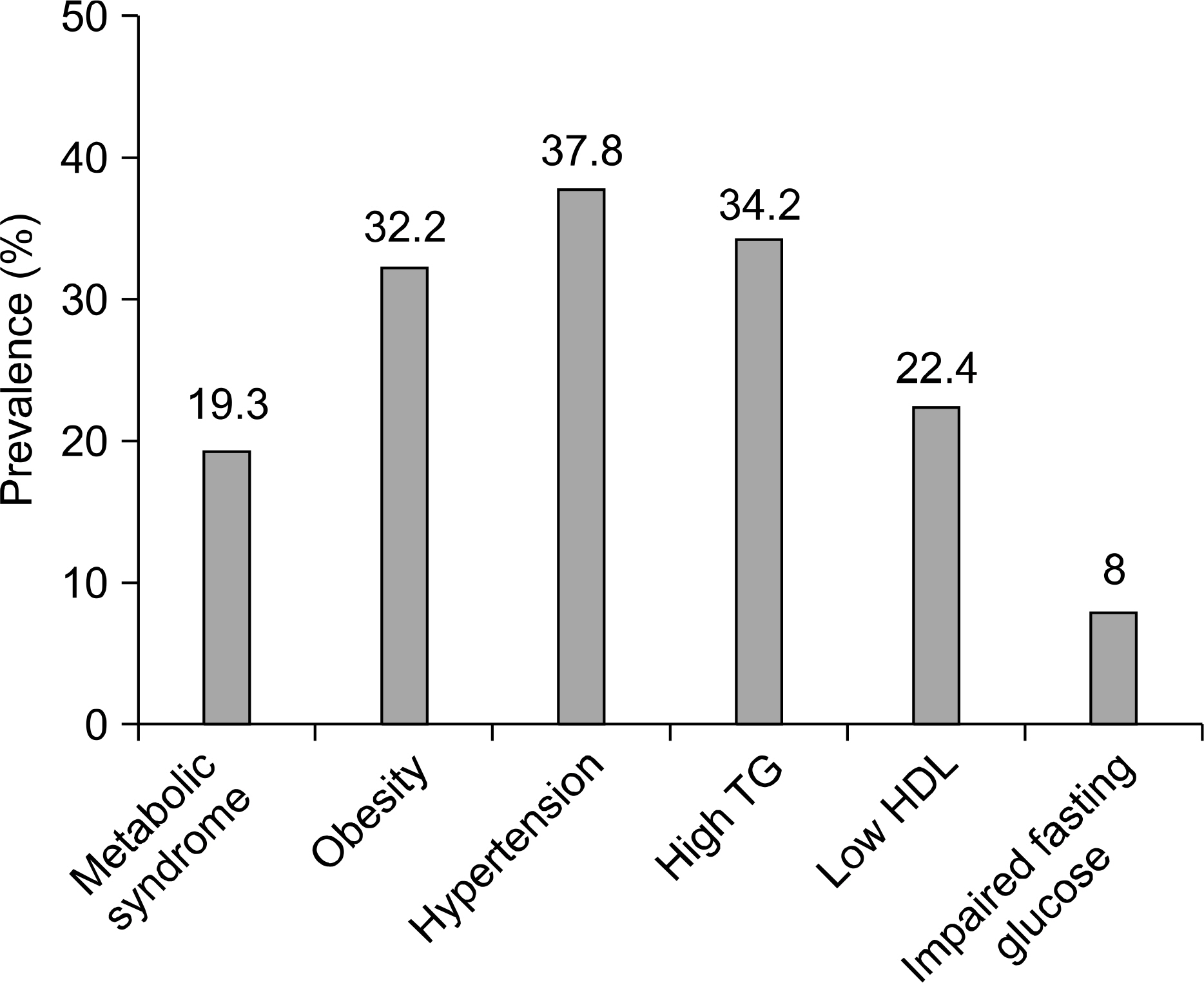
Fig. 2. The prevalence of individual metabolic components. TG: triglyceride, HDL: high-density lipoprotein.

Fig. 3. The prevalence of chronic kidney disease (CKD). CKD was categorized according to the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines. I: GFR≥90 ml/min, II: 60-89 ml/min, III: 30-59 ml/min.
Reference
-
1.Chen J., Muntner P., Hamm LL., Jones DW., Batuman V., Fonseca V, et al. The metabolic syndrome and chronic kidney disease in U.S. adults. Ann Intern Med. 2004. 140:167–74.2.Go AS., Chertow GM., Fan D., McCulloch CE., Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004. 351:1296–305.
Article3.Weiner DE., Tighiouart H., Amin MG., Stark PC., MacLeod B., Griffith JL, et al. Chronic kidney disease as a risk factor for cardiovascular disease and all-cause mortality: a pooled analysis of community-based studies. J Am Soc Nephrol. 2004. 15:1307–15.
Article4.Kurella M., Lo JC., Chertow GM. Metabolic syndrome and the risk for chronic kidney disease among non diabetic adults. J Am Soc Nephrol. 2005. 16:2134–40.5.Kitiyakara C., Yamwong S., Cheepudomwit S., Domrongkitchai-porn S., Unkurapinun N., Pakpeankitvatana V, et al. The metabolic syndrome and chronic kidney disease in a Southeast Asian cohort. Kidney Int. 2007. 71:693–700.
Article6.Tanaka H., Shiohira Y., Uezu Y., Higa A., Iseki K. Metabolic syndrome and chronic kidney disease in Okinawa, Japan. Kidney Int. 2006. 69:369–74.
Article7.Eckel RH., Grundy SM., Zimmet PZ. The metabolic syndrome. Lancet. 2005. 365:1415–28.
Article8.Bagby SP. Obesity-initiated metabolic syndrome and the kidney: a recipe for chronic kidney disease? J Am Soc Nephrol. 2004. 15:2775–91.
Article9.Wilson PW., D'Agostino RB., Levy D., Belanger AM., Silvershatz H., Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation. 1998. 97:1837–47.
Article10.Fuster V., Gotto AM., Libby P., Loscalzo J., McGill HC. 27th Bethesda Conference: matching the intensity of risk factor management with the hazard for coronary disease events. Task Force 1. Pathogenesis of coronary disease: the biologic role of risk factors. J Am Coll Cardiol. 1996. 27:964–76.11.Kim JH., Shim BS., Hong YS. The relating factors of metabolic syndrome to benign prostatic hyperplasia. Korean J Urol. 2005. 46:1046–50.12.Park JS., Park JK. The meaning of metabolic syndrome X in patients suffering with benign prostatic hyperplasia. Korean J Urol. 2007. 48:696–700.
Article13.Kim JH., Shim BS., Kim JS., Hong YS. Voiding dysfunction of men is associated with metabolic syndrome. Korean J Urol. 2006. 47:257–62.
Article14.Humphrey LL., Ballard DJ., Frohnert PP., Chu CP., O'Fallon WM., Palumbo PJ. Chronic renal failure in non-insulin-dependent diabetes mellitus. A population-based study in Rochester, Minnesota. Ann Intern Med. 1989. 111:788–96.15.Brancati FL., Whelton PK., Randall BL., Neaton JD., Stamler J., Klag MJ. Risk of end-stage renal disease in diabetes mellitus: a prospective cohort study of men screened for MRFIT. Multiple Risk Factor Intervention Trial. JAMA. 1997. 278:2069–74.
Article16.Expert panel on detection, evaluation, and treatment of high blood cholesterol in adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol In adults (adult treatment panel III). JAMA. 2001. 285:2486–97.17.Steinbaum SR. The metabolic syndrome: an emerging health epidemic in women. Prog Cardiovasc Dis. 2004. 46:321–36.
Article18.Levey AS., Eckardt KU., Tsukamoto Y., Levin A., Coresh J., Rossert J, et al. Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005. 67:2089–100.
Article19.Abate N., Chandalia M., Cabo-Chan AV Jr., Moe OW., Sakhaee K. The metabolic syndrome and uric acid nephrolithiasis: novel features of renal manifestation of insulin resistance. Kidney Int. 2004. 65:386–92.
Article20.Hanley AJ., Karter AJ., Williams K., Festa A., D'Agostino RB Jr., Wagenknecht LE, et al. Prediction of type 2 diabetes mellitus with alternative definitions of the metabolic syndrome: the Insulin Resistance Atherosclerosis Study. Circulation. 2005. 112:3713–21.21.Fried LF., Orchard TJ., Kasiske BL. Effect of lipid reduction on the progression of renal disease: a meta-analysis. Kidney Int. 2001. 59:260–9.
Article22.Kambham N., Markowitz GS., Valeri AM., Lin J., D'Agati VD. Obesity-related glomerulopathy: an emerging epidemic. Kidney Int. 2001. 59:1498–509.
Article23.Weisinger JR., Kempson RL., Eldridge FL., Swenson RS. The nephrotic syndrome: a complication of massive obesity. Ann Intern Med. 1974. 81:440–7.
Article24.Iseki K., Ikemiya Y., Kinjo K., Inoue T., Iseki C., Takishita S. Body mass index and the risk of development of end-stage renal disease in a screened cohort. Kidney Int. 2004. 65:1870–6.
Article25.Verani RR. Obesity-associated focal segmental glomerulosclerosis: pathological features of the lesion and relationship with cardiomegaly and hyperlipidemia. Am J Kidney Dis. 1992. 20:629–34.
Article26.Kim ES., Han SM., Kim YI., Song KH., Kim MS., Kim WB, et al. Prevalence and clinical characteristics of metabolic syndrome in a rural population of South Korea. Diabet Med. 2004. 21:1141–3.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Can management of the components of metabolic syndrome modify the course of chronic kidney disease?
- The Prevalence of Metabolic Syndrome inthe Chronic Kidney Disease Patients
- Clinical impact of nonalcoholic fatty liver disease on other medical diseases
- Metabolically Healthy Obesity: Epidemiology, Criteria, and Implications in Chronic Kidney Disease
- A case of living-related kidney transplantation in Bartter's syndrome
