J Dent Anesth Pain Med.
2015 Mar;15(1):17-23.
Protective dental splint for oroendotracheal intubation: experience of 202 cases
- Affiliations
-
- 1Department of Advanced General Dentistry, Yonsei University, Seoul, Korea. kdkim@yuhs.ac
- 2Department of Advanced General Dentistry, Dankook University, Cheonan, Korea.
Abstract
- BACKGROUND
Dental injury as a result of oroendotracheal intubation during general anesthesia is very common. We report our experiences of using mouthguard to prevent dental injury during intubation based on our protocol.
METHODS
This retrospective study enrolled patients referred for preanesthetic evaluation, those patients with a history of any of the dental treatments to their anterior teeth listed on our fabrication protocol from January 1, 2009 to June 30, 2010.
RESULTS
No cases of dental trauma during oroendotracheal intubation were reported among the 202 patients who used a protective device. 66% of the patients had risk factors for hard tissue damage aged 10-40 years. At the ages of 40-70 years, the incidence of risk group for periodontal damage was higher.
CONCLUSIONS
Preanesthetic consultation was effective for preventing dental injury, so preanesthetic questionnaire and proper dental consultation would be helpful.
Keyword
MeSH Terms
Figure
-
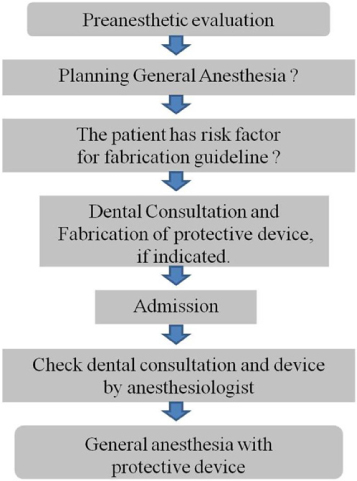
Fig. 1 Critical pathway for the prevention of dental injury during general anesthesia.

Fig. 2 Schematic figures of dental structure. (A) Normal tooth structure, (B) Periodontitis, (C) Root resorption, (D) Root canal treatment (Endodontic treatment).
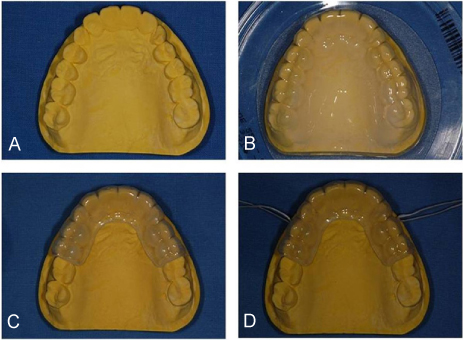
Fig. 3 Mouthguard fabrication procedure.

Fig. 4 The patient's mouth before (A) and after (B) delivery of the mouthguard.
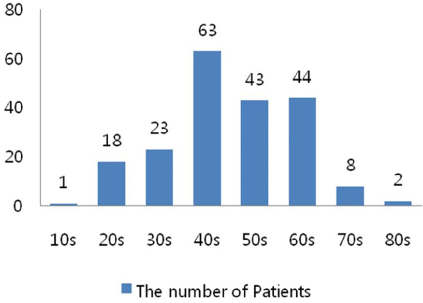
Fig. 5 The distribution of age among the 202 patients in this study.
Reference
-
1. Chen JJ, Susetio L, Chao CC. Oral complications associated with endotracheal general anesthesia. Anaesthesiologica Sinica. 1990; 28:163–169.2. Givol N, Gershtansky Y, Halamish-Shani T, Taicher S, Perel A, Segal E. Perianesthetic dental injuries: Analysis of incident reports. J Clin Anesth. 2004; 16:173–176.
Article3. Lockhart PB, Feldbau EV, Gabel RA, Connolly SF, Silversin JB. Dental complications during and after tracheal intubation. J Am Dent Assoc. 1986; 112:480–483.
Article4. Burton JF, Baker AB. Dental damage during anaesthesia and surgery. Anaesth Intensive Care. 1987; 15:262–268.
Article5. Deppe H, Reeker W, Horch HH, Kochs E. Tooth injury during intubation--diagnostic and therapeutic aspects. Anasthesiol Intensivmed Notfallmed Schmerzther. 1998; 33:722–725.6. Folwaczny M, Hickel R. Oro-dental injuries during intubation anesthesia. Anaesthesist. 1998; 47:707–731.7. Magnin C, Bory EN, Motin J. Tooth injuries during intubation: a new preventive device. Ann Fr Anesth Reanim. 1991; 10:171–174.8. Warner ME, Benenfeld SM, Warner MA, Schroeder DR, Maxson PM. Perianesthetic dental injuries: Frequency, outcomes, and risk factors. Anesthesiology. 1999; 90:1302–1305.
Article9. Owen H, Waddell-Smith I. Dental trauma associated with anaesthesia. Anaesth Intensive Care. 2000; 28:133–145.
Article10. Cass NM. Medicolegal claims against anaesthetists: A 20 year study. Anaesth Intensive Care. 2004; 32:47–58.
Article11. Newland MC, Ellis SJ, Peters KR, Simonson JA, Durham TM, Ullrich FA, et al. Dental injury associated with anesthesia: A report of 161,687 anesthetics given over 14 years. J Clin Anesth. 2007; 19:339–345.
Article12. Chadwick RG, Lindsay SM. Dental injuries during general anaesthesia. Br Dent J. 1996; 180:255–258.
Article13. Hagelsten JO, Marvitz L. Prevention of dental damage during anesthesia. Z Prakt Anasth. 1971; 6:195–205.14. Ghabash MB, Matta MS, Mehanna CB. Prevention of dental trauma during endotracheal intubation. Anesth Analg. 1997; 84:230–231.
Article15. Haddy S. Protecting teeth during endotracheal intubation. Anesthesiology. 1989; 71:810–811.
Article16. Sato N, Shingu K. Another reason to choose the left molar approach of laryngoscopy: To spare the incisor teeth. Anesthesiology. 2002; 96:1279.
Article17. Monaca E, Fock N, Doehn M, Wappler F. The effectiveness of preformed tooth protectors during endotracheal intubation: An upper jaw model. Anesth Analg. 2007; 105:1326–1332.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Modified submental approach to oroendotracheal intubation in patients with panfacial bone fractures
- Creating protective appliances for preventing dental injury during endotracheal intubation using intraoral scanning and 3D printing: a technical note
- Flexible laryngeal mask airway management for dental treatment cases associated with difficult intubation
- Orotracheal intubation in a patient with difficult airway by using fiberoptic nasotracheal intubation: A case report
- Treatment and Clinical Application Of a Triangular Splint Method for Fracture of the Humerus
