Sonoanatomical Change of Phrenic Nerve According to Posture During Ultrasound-Guided Stellate Ganglion Block
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Korea University Guro Hospital, Seoul, Korea. rehab46@korea.ac.kr
- KMID: 2309923
- DOI: http://doi.org/10.5535/arm.2016.40.2.244
Abstract
OBJECTIVE
To evaluate the risk of phrenic nerve injury during ultrasound-guided stellate ganglion block (US-SGB) according to sonoanatomy of the phrenic nerve, and determine a safer posture for needle insertion by assessing its relationship with surrounding structure according to positional change.
METHODS
Twenty-nine healthy volunteers were recruited and underwent ultrasound in two postures, i.e., supine position with the neck extension and head rotation, and lateral decubitus position. The transducer was placed at the anterior tubercle of the C6 level to identify phrenic nerve. The cross-sectional area (CSA), depth from skin, distance between phrenic nerve and anterior tubercle of C6 transverse process, and the angle formed by anterior tubercle, posterior tubercle and phrenic nerve were measured.
RESULTS
The phrenic nerve was clearly identified in the intermuscular fascia layer between the anterior scalene and sternocleidomastoid muscles. The distance between the phrenic nerve and anterior tubercle was 10.33±3.20 mm with the supine position and 9.20±3.31 mm with the lateral decubitus position, respectively. The mean CSA and skin depth of phrenic nerve were not statistically different between the two positions. The angle with the supine position was 48.37°±27.43°, and 58.89°±30.02° with the lateral decubitus position. The difference of angle between the two positions was statistically significant.
CONCLUSION
Ultrasound is a useful tool for assessing the phrenic nerve and its anatomical relation with other cervical structures. In addition, lateral decubitus position seems to be safer by providing wider angle for needle insertion than the supine position in US-SGB.
Keyword
MeSH Terms
Figure
-
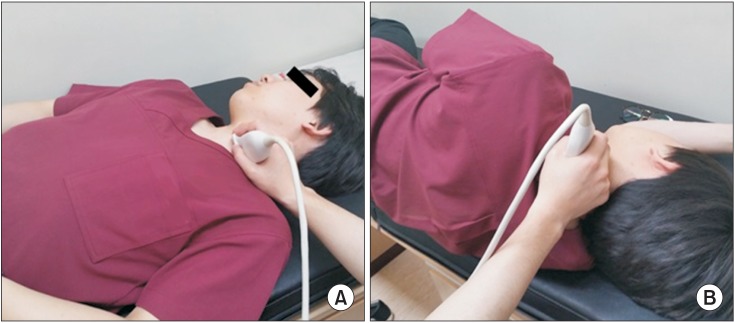
Fig. 1 Sonographic evaluations were performed in two postures. (A) Supine position with the neck slightly extended, and the head rotated slightly to the opposite side to be blocked. (B) Lateral decubitus position with the side to be treated uppermost.
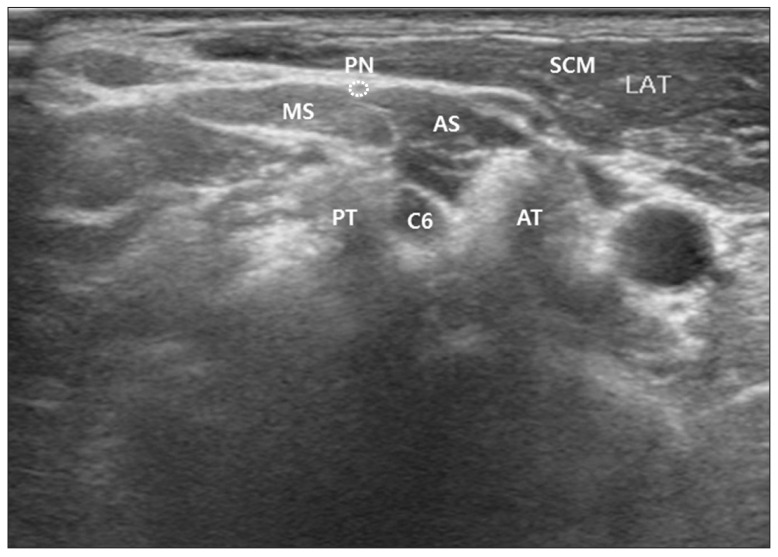
Fig. 2 Sonographic landmarks, anterior scalene muscle (AS), middle scalene muscle (MS), sternocleidomastoid muscle (SCM), anterior tubercle (AT), and phrenic nerve (PN), were identified on the plane of vertebral C6 level. The margin of phrenic nerve was presented as dotted line. C6, C6 nerve root; PT, posterior tubercle.
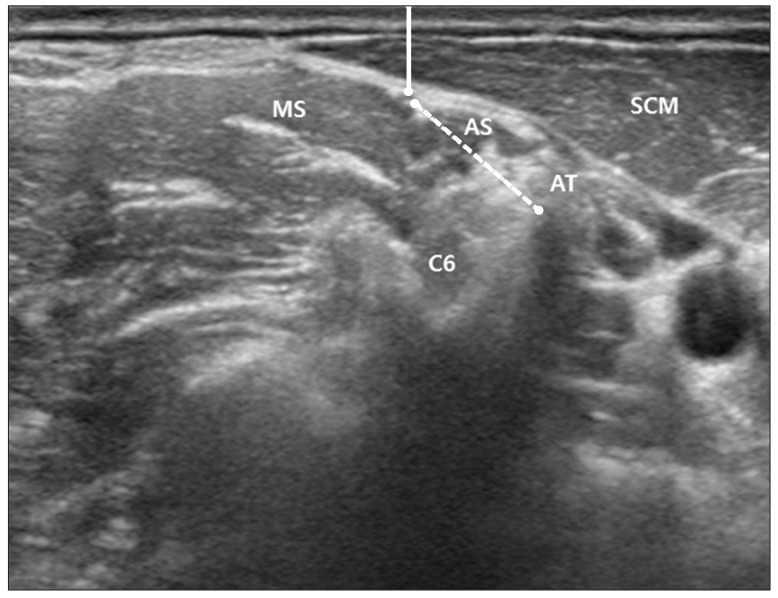
Fig. 3 Depth of phrenic nerve from skin was measured by the shortest distance between the epineurium of phrenic nerve and the surface of skin (presented as solid line). The shortest distance between the epineurium of phrenic nerve and the anterior tubercle (AT) of the C6 transverse process was also measured (presented as dotted line). SCM, sternocleidomastoid muscle; AS, anterior scalene muscle; MS, middle scalene muscle; C6, C6 nerve root.
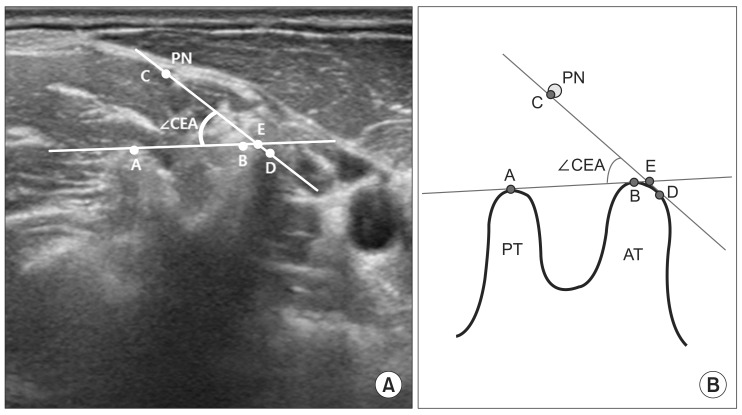
Fig. 4 The angle formed by the lower margin of epineurium of PN (point 'C'), point 'E', and the upper margin of PT (point 'A') (∠CEA) was described on ultrasound image (A) and schematic image (B). 'A', upper margin of PT; 'B', point on the AT created by connecting PT and AT; 'C', lower margin of epineurium of PN; 'D', point on the AT created by connecting lower margin of PN and AT; 'E', crossed point of extended line AB and CD; PN, phrenic nerve; PT, posterior tubercle; AT, anterior tubercle.
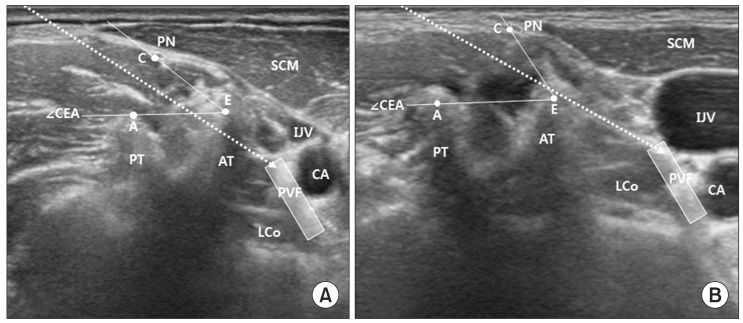
Fig. 5 Virtual needle pathways were described as dotted arrows. The target point was represented as shaded rectangle. (A) When the safe angle (∠CEA) is small, if the needle aims at the target point directly, the needle would be blocked by AT and cannot reach the target point. (B) When the needle pathway is positioned within the range of safe angle (∠CEA), the needle could reach the target point without contacting the AT and PN. Larger safe angle (∠CEA) provides greater possibility to approach the target point safely. 'A', upper margin of PT; 'C', lower margin of epineurium of PN; 'E', crossed point of extended line AB and CD; AT, anterior tubercle; PN, phrenic nerve; PT, posterior tubercle; IJV, internal jugular vein; CA, carotid artery; PVF, prevertebral fascia; LCo, longus colli muscle.
Reference
-
1. Elias M. Cervical sympathetic and stellate ganglion blocks. Pain Physician. 2000; 3:294–304. PMID: 16906187.
Article2. Kessler J, Schafhalter-Zoppoth I, Gray AT. An ultrasound study of the phrenic nerve in the posterior cervical triangle: implications for the interscalene brachial plexus block. Reg Anesth Pain Med. 2008; 33:545–550. PMID: 19258969.
Article3. Canella C, Demondion X, Delebarre A, Moraux A, Cotten H, Cotten A. Anatomical study of phrenic nerve using ultrasound. Eur Radiol. 2010; 20:659–665. PMID: 19727747.
Article4. Gofeld M, Bhatia A, Abbas S, Ganapathy S, Johnson M. Development and validation of a new technique for ultrasound-guided stellate ganglion block. Reg Anesth Pain Med. 2009; 34:475–479. PMID: 19920422.
Article5. Narouze SN. Ultrasound-guided cervical spine injections: ultrasound "prevents" whereas contrast fluoroscopy "detects" intravascular injections. Reg Anesth Pain Med. 2012; 37:127–130. PMID: 22354064.6. Narouze SN, Vydyanathan A, Kapural L, Sessler DI, Mekhail N. Ultrasound-guided cervical selective nerve root block: a fluoroscopy-controlled feasibility study. Reg Anesth Pain Med. 2009; 34:343–348. PMID: 19574867.7. Saranteas T, Paraskeuopoulos T, Anagnostopoulou S, Kanellopoulos I, Mastoris M, Kostopanagiotou G. Ultrasound anatomy of the cervical paravertebral space: a preliminary study. Surg Radiol Anat. 2010; 32:617–622. PMID: 20082079.
Article8. Siegenthaler A, Mlekusch S, Schliessbach J, Curatolo M, Eichenberger U. Ultrasound imaging to estimate risk of esophageal and vascular puncture after conventional stellate ganglion block. Reg Anesth Pain Med. 2012; 37:224–227. PMID: 22157739.
Article9. Abdi S, Zhou Y, Patel N, Saini B, Nelson J. A new and easy technique to block the stellate ganglion. Pain Physician. 2004; 7:327–331. PMID: 16858470.
Article10. Wallace MS, Milholland AV. Contralateral spread of local anesthetic withstellate ganglion block. Reg Anesth. 1993; 18:55–59. PMID: 8095400.11. Mak PH, Irwin MG, Ooi CG, Chow BF. Incidence of diaphragmatic paralysis following supraclavicular brachial plexus block and its effect on pulmonary function. Anaesthesia. 2001; 56:352–356. PMID: 11284823.
Article12. Robaux S, Bouaziz H, Boisseau N, Raucoules-Aime M, Laxenaire MC. S.O.S. Regional Hot Line Service. Persistent phrenic nerve paralysis following interscalene brachial plexus block. Anesthesiology. 2001; 95:1519–1521. PMID: 11748414.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bilateral Horner's Syndrome after a Stellate Ganglion Block
- Computerized Tomography - guided Percutaneous Radiofrequency
- Stellate Ganglion Block for the Treatment of Classic Migraine: A case report
- Thermographic Follow up of the Stellate Ganglion Block: Case Report
- Ultrasound-Guided Pain Interventions: A Review of Techniques for Peripheral Nerves
