A Dual (Brachial and Contralateral Femoral) Approach for Subintimal Angioplasty of Long Ilio-Femoral Occlusive Disease Including the Iliac Ostium
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Kyung Hee University Medical Center, Seoul, Korea. mylovekw@hanmail.net
- KMID: 2297945
- DOI: http://doi.org/10.4070/kcj.2010.40.2.90
Abstract
- As techniques and device technology have improved, the success rates and long patency of ilio-femoral occlusive disease have also improved. In the case of extensive iliac occlusive disease, however, wire passage and handling remain a challenge due to the relatively weak guiding catheter backup support with the contralateral femoral approach. There has been no report on methods to overcome this problem. We performed a successful percutaneous translunimal angioplasty for long ilio-femoral occlusive disease including the iliac ostium by a dual approach including simultaneous brachial and contralateral femoral arteries for subintimal angioplasty.
Figure
-

Fig. 1 Computed tomography-angiography (CTA) of the lower extremity. (A) shows total occlusion from the left common iliac artery ostium to the distal femoral artery with a reasonably collateralized circulation; after percutaneous transluminal angioplasty, the follow-up CTA revealed no residual stenosis from the common iliac artery to the distal femoral artery as shown in (B).
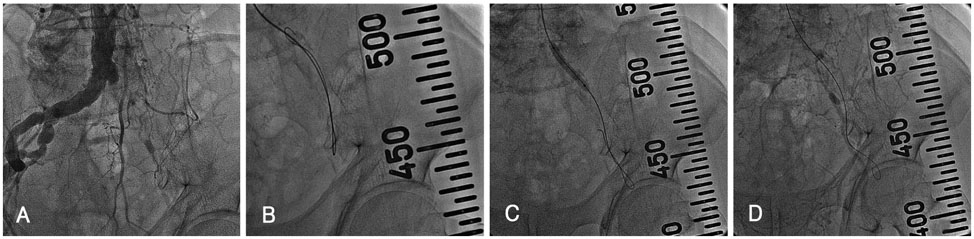
Fig. 2 Subintimal wiring for iliac occlusion through right brachial artery. Lower limb angiography via the right brachial artery revealed total occlusion of the left common iliac artery and left common femoral artery with collateral flow that reconstructed the distal superficial femoral artery as shown in (A). Using a 0.035 inch angled Terumo wire with a backup catheter; successful wiring from the common iliac artery to the external iliac artery was performed by subintimal wire tracking as shown in (B). After predilation (C), subintimal dye staining was noted as shown in (D).
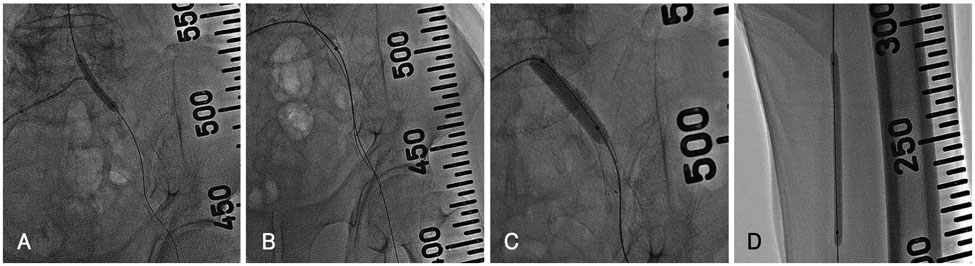
Fig. 3 Subintimal wiring for superficial femoral artery occlusion via the contralateral femoral artery. A six French Balkin sheath was inserted through the contralateral femoral artery (A), and a 0.035 inch angled Terumo wire was successfully passed through the superficial femoral artery by the antegrade approach via the right femoral artery (B). A 10.0×60 mm peripheral self-expandable stent (Smart, Cordis) was deployed in the common iliac artery to the external iliac artery (C). Percutaneous transluminal angioplasty for the common iliac artery and superficial femoral artery was carried out (D).
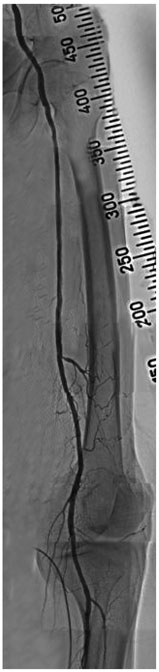
Fig. 4 Final angiography. After percutaneous transluminal angioplasty, patent stents with good distal flow were noted.
Reference
-
1. Dormandy JA, Rutherford RB. Management of peripheral arterial disease (PAD): TransAtlantic InterSociety Consensus (TASC). J Vasc Surg. 2000. 31:S1–S296.2. Rutherford RB. Options in the surgical management of aortoiliac occlusive disease: a changing perspective. Cardiovasc Surg. 1999. 7:5–12.3. Whiteley MS, Ray-Chaudhuri SB, Galland RB. Changing patterns in aortoiliac reconstruction: a 7-year audit. Br J Surg. 1996. 83:1367–1369.4. Upchurch GR, Dimick JB, Wainess RM, et al. Diffusion of new technology in health care: the case of aorto-iliac occlusive disease. Surgery. 2004. 136:812–818.5. Kashyap VS, Pavkov ML, Bena JF, et al. The management of severe aortoiliac occlusive disease: endovascular therapy rivals open reconstruction. J Vasc Surg. 2008. 48:1451–1457.6. Dyet JF, Gaines PA, Nicholson AA, et al. Treatment of chronic iliac artery occlusions by means of percutaneous endovascular stent placement. J Vasc Interv Radiol. 1997. 8:349–353.7. Henry M, Amor M, Ethevenot G, Henry I, Mentre B, Tzvetanov K. Percutaneous endoluminal treatment of iliac occlusions: long term follow-up in 105 patients. J Endovasc Surg. 1998. 5:228–235.8. Uher P, Nyman U, Lindh M, Lindblad B, Ivancev K. Long-term results for stenting chronic iliac artery occlusions. J Endovasc Ther. 2002. 9:67–75.9. Carnevale FC, De Blas M, Merino S, Egana JM, Caldas JG. Percutaneous endovascular treatment of chronic iliac artery occlusion. Cardiovasc Intervent Radiol. 2004. 27:447–452.10. Lee SH, Park HS, Jang SY, et al. A case of peripheral revascularization via the radial artery using devices designed for percutaneous coronary intervention. Korean Circ J. 2008. 38:671–673.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful Recanalization of a Long Superficial Femoral Artery Occlusion by Retrograde Subintimal Angioplasty After a Failed Antegrade Subintimal Approach
- Subintimal Stent Placement in Patients with Long Segment Occlusion of the Iliac Artery
- Endovascular Management for Chronic Steno-occlusion of Iliac and Femoral Arteries
- Effects of Subintimal Angioplasty in Patients with Ischemic Arterial Disease of Lower Extremities
- The Relation between Distal Runoff and Clinical Outcome after Aorto-iliac Reconstruction Surgery
