Management of Organic Mitral Regurgitation: Guideline Recommendations and Controversies
- Affiliations
-
- 1Cardiology Department, University of Medicine and Pharmacy "Carol Davila", Bucharest, Romania. bogdan.a.popescu@gmail.com
- 2Cardiology Department, Emergency Institute for Cardiovascular Diseases "Prof. Dr. C. C. Iliescu", Bucharest, Romania.
- 3Cardiology Department, Emergency University Hospital Elias, Bucharest, Romania.
- KMID: 2297874
- DOI: http://doi.org/10.4070/kcj.2015.45.2.96
Abstract
- Mitral regurgitation (MR) represents the second most frequent valvular heart disease. The appropriate management of organic MR remains unclear in many aspects, especially in several specific clinical scenarios. This review aims to discuss the current guideline recommendations regarding the management of organic MR, while highlighting the controversial aspects encountered in daily clinical practice. The role of imaging is essential in establishing the most appropriate type of surgical treatment (repair or replace), which is based on morphological mitral valve (MV) characteristics (reparability of the valve) and local surgical expertise in valve repair. The potential advantages of 3-dimensional echocardiography in assessing the MV are discussed. Other modern imaging techniques (tissue Doppler and speckle tracking) may provide additional useful information in borderline cases. Exercise echocardiography (evaluating MR severity, pulmonary pressure, or right ventricular function) may have an important role in the management of difficult cases. Finally, the moment when surgery is no longer an option and alternative solutions should be sought is also discussed. Although in everyday clinical practice the timing of surgery is not always straightforward, some newer clinical and echocardiographic indicators can guide this decision and help improve the outcome of these patients.
MeSH Terms
Figure
-

Fig. 1 Mitral valve lesions in severe organic mitral regurgitation, assessed by three-dimensional transoesophageal echocardiography. A: severe mitral regurgitation determined by a simple lesion with a high probability of successful mitral valve repair. 3D transoesophageal surgical view of the mitral valve showing isolated P2 scallop prolapse (asterisk) (Supplementary Video 1 in the online-only Data Supplement). B: severe mitral regurgitation determined by complex lesions with a possibly successful mitral valve repair by an experienced surgeon. 3D transoesophageal surgical view of the mitral valve showing P3 scallop prolapse and flail (asterisk) involving the posterior commissure (Supplementary Video 2 in the online-only Data Supplement). C: severe mitral regurgitation determined by a very complex lesion with an unlikely chance of successful mitral valve repair. 3D transoesophageal surgical view in a patient with Barlow disease and P2 flail (asterisk) (Supplementary Video 3 in the online-only Data Supplement). 3D: three-dimensional.
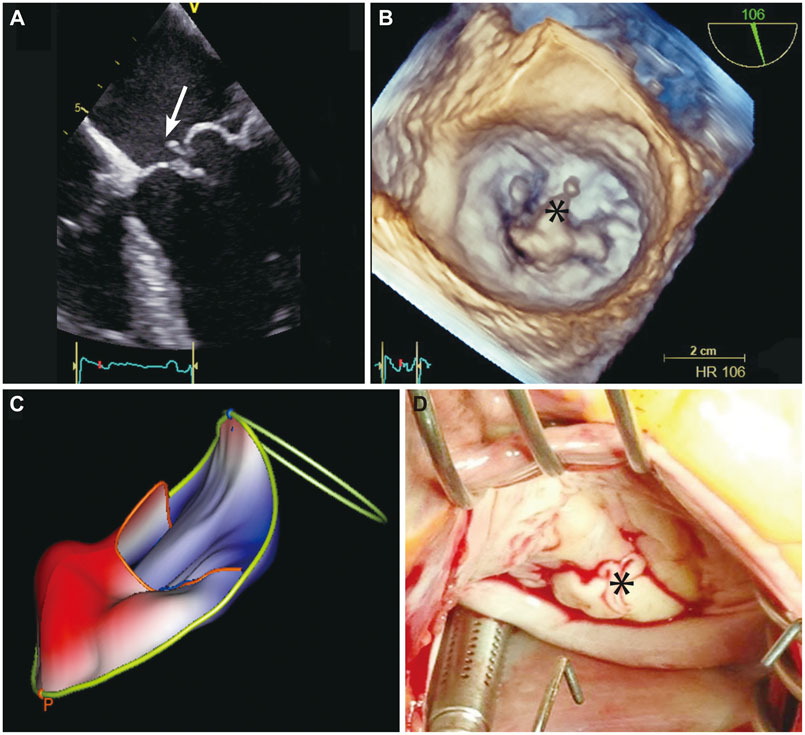
Fig. 2 Mitral valve assessment in a patient with severe mitral regurgitation. A: 2D transoesophageal four chamber view of posterior mitral valve prolapse and flail due to chordal rupture (arrow) (Supplementary Video 4 in the online-only Data Supplement). B: 3D transoesophageal view of the mitral valve seen from the left atrium showing isolated P2 prolapse and flail (asterisk) (Supplementary Video 5 in the online-only Data Supplement). C: 3D mitral valve reconstruction demonstrating P2 prolapse (color coded in red). D: intraoperative findings confirming the echo results: P2 scallop chordal rupture (asterisk). 2D: two-dimensional, 3D: three-dimensional.

Fig. 3 Mitral valve reconstruction in a normal subject (A) and in a patient with severe mitral regurgitation due to P2 scallop flail and prolapse and P3 scallop prolapse (B). The parts of the mitral valve which are below the mitral annulus plane (i.e., on the ventricular side) are color-coded in blue, while the parts which are above annulus are coded in red. Of note, the shape of the mitral annulus changes in MR, becoming circular (B), compared to the oval shape of the normal mitral annulus (A). MR: metral regurgitation.
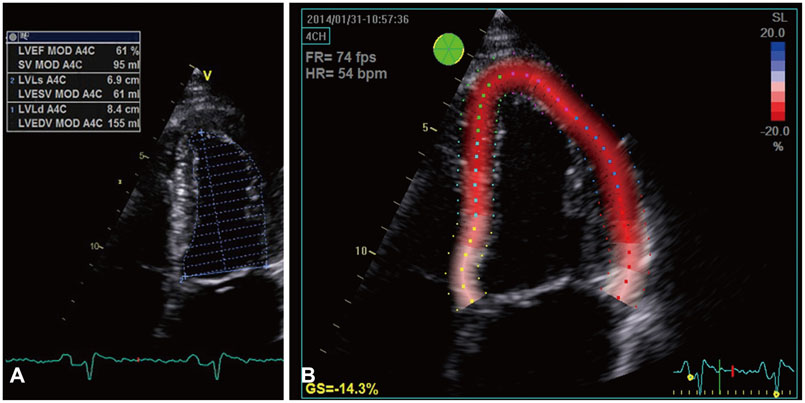
Fig. 4 Echocardiographic images from a patient with severe asymptomatic mitral regurgitation. There is a preserved left ventricular (LV) ejection fraction calculated by Simpson's method (61%) (A), but reduced global longitudinal strain (-14.3%) (B), suggesting subclinical LV systolic dysfunction (Supplementary Video 6 in the online-only Data Supplement). LVEF: left ventricular ejection fraction, SV: stroke volume, LVESV: left ventricular end systolic volume, LVEDV: left ventricular end diastolic volume.

Fig. 5 Left atrium (LA) function evaluation in a patient with severe asymptomatic mitral regurgitation (MR). The LA ejection fraction calculated by LA maximum volume (130 mL in A)-LA minimum volume (80 mL in B) divided by LA maximum volume is decreased to 38%. The LA strain values (i.e., reservoir, conduit, and contractile function) calculated by speckle tracking imaging (C) in the same patient with severe asymptomatic MR are decreased.
Reference
-
1. Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003; 24:1231–1243.2. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006; 368:1005–1011.3. Delahaye JP, Gare JP, Viguier E, Delahaye F, De Gevigney G, Milon H. Natural history of severe mitral regurgitation. Eur Heart J. 1991; 12:Suppl B. 5–9.4. Tribouilloy CM, Enriquez-Sarano M, Schaff HV, et al. Impact of preoperative symptoms on survival after surgical correction of organic mitral regurgitation: rationale for optimizing surgical indications. Circulation. 1999; 99:400–405.5. Enriquez-Sarano M, Schaff HV, Orszulak TA, Tajik AJ, Bailey KR, Frye RL. Valve repair improves the outcome of surgery for mitral regurgitation. A multivariate analysis. Circulation. 1995; 91:1022–1028.6. Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014; 63:2438–2488.7. Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC). European Association for Cardio-Thoracic Surgery (EACTS). Vahanian A, et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J. 2012; 33:2451–2496.8. Gammie JS, Sheng S, Griffith BP, et al. Trends in mitral valve surgery in the United States: results from the Society of Thoracic Surgeons Adult Cardiac Surgery Database. Ann Thorac Surg. 2009; 87:1431–1437. discussion 1437-9.9. Castillo JG, Anyanwu AC, Fuster V, Adams DH. A near 100% repair rate for mitral valve prolapse is achievable in a reference center: implications for future guidelines. J Thorac Cardiovasc Surg. 2012; 144:308–312.10. Castillo JG, Anyanwu AC, El-Eshmawi A, Adams DH. All anterior and bileaflet mitral valve prolapses are repairable in the modern era of reconstructive surgery. Eur J Cardiothorac Surg. 2014; 45:139–145. discussion 145.11. Gammie JS, O'Brien SM, Griffith BP, Ferguson TB, Peterson ED. Influence of hospital procedural volume on care process and mortality for patients undergoing elective surgery for mitral regurgitation. Circulation. 2007; 115:881–887.12. Bolling SF, Li S, O'Brien SM, Brennan JM, Prager RL, Gammie JS. Predictors of mitral valve repair: clinical and surgeon factors. Ann Thorac Surg. 2010; 90:1904–1911. discussion 1912.13. Omran AS, Woo A, David TE, Feindel CM, Rakowski H, Siu SC. Intraoperative transesophageal echocardiography accurately predicts mitral valve anatomy and suitability for repair. J Am Soc Echocardiogr. 2002; 15:950–957.14. Lancellotti P, Tribouilloy C, Hagendorff A, et al. Recommendations for the echocardiographic assessment of native valvular regurgitation: an executive summary from the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2013; 14:611–644.15. De Bonis M, Bolling SF. Mitral valve surgery: wait and see vs. early operation. Eur Heart J. 2013; 34:13–19a.16. Vegas A, Meineri M. Core review: three-dimensional transesophageal echocardiography is a major advance for intraoperative clinical management of patients undergoing cardiac surgery: a core review. Anesth Analg. 2010; 110:1548–1573.17. Pepi M, Tamborini G, Maltagliati A, et al. Head-to-head comparison of two- and three-dimensional transthoracic and transesophageal echocardiography in the localization of mitral valve prolapse. J Am Coll Cardiol. 2006; 48:2524–2530.18. Shanks M, Siebelink HM, Delgado V, et al. Quantitative assessment of mitral regurgitation: comparison between three-dimensional transesophageal echocardiography and magnetic resonance imaging. Circ Cardiovasc Imaging. 2010; 3:694–700.19. Rosenhek R, Rader F, Klaar U, et al. Outcome of watchful waiting in asymptomatic severe mitral regurgitation. Circulation. 2006; 113:2238–2244.20. Kang DH, Kim JH, Rim JH, et al. Comparison of early surgery versus conventional treatment in asymptomatic severe mitral regurgitation. Circulation. 2009; 119:797–804.21. Suri RM, Vanoverschelde JL, Grigioni F, et al. Association between early surgical intervention vs watchful waiting and outcomes for mitral regurgitation due to flail mitral valve leaflets. JAMA. 2013; 310:609–616.22. Tietge WJ, de Heer LM, van Hessen MW, et al. Early mitral valve repair versus watchful waiting in patients with severe asymptomatic organic mitral regurgitation; rationale and design of the Dutch AMR trial, a multicenter, randomised trial. Neth Heart J. 2012; 20:94–101.23. Kang DH, Park SJ, Sun BJ, et al. Early surgery versus conventional treatment for asymptomatic severe mitral regurgitation: a propensity analysis. J Am Coll Cardiol. 2014; 63:2398–2407.24. Pizarro R, Bazzino OO, Oberti PF, et al. Prospective validation of the prognostic usefulness of brain natriuretic peptide in asymptomatic patients with chronic severe mitral regurgitation. J Am Coll Cardiol. 2009; 54:1099–1106.25. Detaint D, Messika-Zeitoun D, Avierinos JF, et al. B-type natriuretic peptide in organic mitral regurgitation: determinants and impact on outcome. Circulation. 2005; 111:2391–2397.26. Klaar U, Gabriel H, Bergler-Klein J, et al. Prognostic value of serial B-type natriuretic peptide measurement in asymptomatic organic mitral regurgitation. Eur J Heart Fail. 2011; 13:163–169.27. Magne J, Mahjoub H, Pierard LA, et al. Prognostic importance of brain natriuretic peptide and left ventricular longitudinal function in asymptomatic degenerative mitral regurgitation. Heart. 2012; 98:584–591.28. Magne J, Mahjoub H, Pibarot P, Pirlet C, Pierard LA, Lancellotti P. Prognostic importance of exercise brain natriuretic peptide in asymptomatic degenerative mitral regurgitation. Eur J Heart Fail. 2012; 14:1293–1302.29. Reisner SA, Lysyansky P, Agmon Y, Mutlak D, Lessick J, Friedman Z. Global longitudinal strain: a novel index of left ventricular systolic function. J Am Soc Echocardiogr. 2004; 17:630–633.30. Beladan CC, Călin A, Roşca M, Ginghină C, Popescu BA. Left ventricular twist dynamics: principles and applications. Heart. 2014; 100:731–740.31. Mascle S, Schnell F, Thebault C, et al. Predictive value of global longitudinal strain in a surgical population of organic mitral regurgitation. J Am Soc Echocardiogr. 2012; 25:766–772.32. Witkowski TG, Thomas JD, Debonnaire PJ, et al. Global longitudinal strain predicts left ventricular dysfunction after mitral valve repair. Eur Heart J Cardiovasc Imaging. 2013; 14:69–76.33. Pandis D, Sengupta PP, Castillo JG, et al. Assessment of longitudinal myocardial mechanics in patients with degenerative mitral valve regurgitation predicts postoperative worsening of left ventricular systolic function. J Am Soc Echocardiogr. 2014; 27:627–638.34. Moustafa SE, Kansal M, Alharthi M, Deng Y, Chandrasekaran K, Mookadam F. Prediction of incipient left ventricular dysfunction in patients with chronic primary mitral regurgitation: a velocity vector imaging study. Eur J Echocardiogr. 2011; 12:291–298.35. Borg AN, Harrison JL, Argyle RA, Ray SG. Left ventricular torsion in primary chronic mitral regurgitation. Heart. 2008; 94:597–603.36. Rusinaru D, Tribouilloy C, Grigioni F, et al. Left atrial size is a potent predictor of mortality in mitral regurgitation due to flail leaflets: results from a large international multicenter study. Circ Cardiovasc Imaging. 2011; 4:473–481.37. Le Tourneau T, Messika-Zeitoun D, Russo A, et al. Impact of left atrial volume on clinical outcome in organic mitral regurgitation. J Am Coll Cardiol. 2010; 56:570–578.38. Ring L, Rana BS, Wells FC, Kydd AC, Dutka DP. Atrial function as a guide to timing of intervention in mitral valve prolapse with mitral regurgitation. JACC Cardiovasc Imaging. 2014; 7:225–232.39. Bonow RO. Left atrial function in mitral regurgitation: guilt by association. JACC Cardiovasc Imaging. 2014; 7:233–235.40. Cameli M, Lisi M, Righini FM, et al. Usefulness of atrial deformation analysis to predict left atrial fibrosis and endocardial thickness in patients undergoing mitral valve operations for severe mitral regurgitation secondary to mitral valve prolapse. Am J Cardiol. 2013; 111:595–601.41. Ghoreishi M, Evans CF, DeFilippi CR, et al. Pulmonary hypertension adversely affects short- and long-term survival after mitral valve operation for mitral regurgitation: implications for timing of surgery. J Thorac Cardiovasc Surg. 2011; 142:1439–1452.42. Barbieri A, Bursi F, Grigioni F, et al. Prognostic and therapeutic implications of pulmonary hypertension complicating degenerative mitral regurgitation due to flail leaflet: a multicenter long-term international study. Eur Heart J. 2011; 32:751–759.43. Crawford FA Jr. Residual pulmonary artery hypertension after mitral valve replacement: size matters! J Am Coll Cardiol. 2005; 45:1041–1042.44. Li M, Dumesnil JG, Mathieu P, Pibarot P. Impact of valve prosthesis-patient mismatch on pulmonary arterial pressure after mitral valve replacement. J Am Coll Cardiol. 2005; 45:1034–1040.45. Walls MC, Cimino N, Bolling SF, Bach DS. Persistent pulmonary hypertension after mitral valve surgery: does surgical procedure affect outcome? J Heart Valve Dis. 2008; 17:1–9. discussion 9.46. Magne J, Lancellotti P, O'Connor K, Van de Heyning CM, Szymanski C, Piérard LA. Prediction of exercise pulmonary hypertension in asymptomatic degenerative mitral regurgitation. J Am Soc Echocardiogr. 2011; 24:1004–1012.47. Magne J, Lancellotti P, Piérard LA. Exercise pulmonary hypertension in asymptomatic degenerative mitral regurgitation. Circulation. 2010; 122:33–41.48. Haddad F, Doyle R, Murphy DJ, Hunt SA. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation. 2008; 117:1717–1731.49. Shiran A, Sagie A. Tricuspid regurgitation in mitral valve disease incidence, prognostic implications, mechanism, and management. J Am Coll Cardiol. 2009; 53:401–408.50. Kusunose K, Popović ZB, Motoki H, Marwick TH. Prognostic significance of exercise-induced right ventricular dysfunction in asymptomatic degenerative mitral regurgitation. Circ Cardiovasc Imaging. 2013; 6:167–176.51. Sürder D, Pedrazzini G, Gaemperli O, et al. Predictors for efficacy of percutaneous mitral valve repair using the MitraClip system: the results of the MitraSwiss registry. Heart. 2013; 99:1034–1040.52. Messika-Zeitoun D. Percutaneous mitral valve repair using the Mitra-Clip system: time to move forward. Heart. 2013; 99:975–976.53. Alfieri O, Maisano F, De Bonis M, et al. The double-orifice technique in mitral valve repair: a simple solution for complex problems. J Thorac Cardiovasc Surg. 2001; 122:674–681.54. De Bonis M, Maisano F, La Canna G, Alfieri O. Treatment and management of mitral regurgitation. Nat Rev Cardiol. 2011; 9:133–146.55. Guarracino F, Baldassarri R, Ferro B, et al. Transesophageal echocardiography during MitraClip® procedure. Anesth Analg. 2014; 118:1188–1196.56. Feldman T, Wasserman HS, Herrmann HC, et al. Percutaneous mitral valve repair using the edge-to-edge technique: six-month results of the EVEREST Phase I Clinical Trial. J Am Coll Cardiol. 2005; 46:2134–2140.57. Feldman T, Foster E, Glower DD, et al. Percutaneous repair or surgery for mitral regurgitation. N Engl J Med. 2011; 364:1395–1406.58. Mauri L, Foster E, Glower DD, et al. 4-year results of a randomized controlled trial of percutaneous repair versus surgery for mitral regurgitation. J Am Coll Cardiol. 2013; 62:317–328.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Echocardiographic Assessment of Mitral Valve Regurgitation
- Assessment of Mitral Stenosis by Doppler Echocardiography: Influence of Regurgitation on Doppler Pressure Half-Time
- Clinical Use of Doppler Echocardiography in Organic Mitral Regurgitation: From Diagnosis to Patients' Management
- Mitral Valve Repair
- Transaortic Mitral Commissuroplasty with a Bentall Procedure or Artic Valve Replacement
