A Case of Allergic Fungal Rhinosinusitis with Concurrently Occuring Fungus Ball
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, School of Medicine, Chungnam National University, Daejeon, Korea. entkym@cnu.ac.kr
- KMID: 2297555
- DOI: http://doi.org/10.18787/jr.2015.22.1.47
Abstract
- Allergic fungal rhinosinusitis (AFRS) is a noninvasive fungal infection of the paranasal sinuses that are usually seen in young immunocompetent patients with atopy and/or asthma. Fungus balls can grow in moist cavities of the paranasal sinuses of a host with normal immunologic status. Cases of AFRS with concurrent fungus balls is very rare. We present a case of a patient who had AFRS on one side of the paranasal sinus and allergic fungal sinusitis on the other side. A 51-year-old female with atopy presented with a few-year history of nasal obstruction and rhinorrhea, as well as a history of high-dose systemic steroid therapy. The patient had nasal polyps and showed an elevated level of total IgE and positive MAST to fungal antigens. Endoscopic sinus surgery was performed. Allergic mucin from the right maxillary sinus contained sheets of eosinophils and Charcot-Leyden crystals. Also, a clay-like dark brown material from the left maxillary sinus was revealed to be a fungus ball.
Keyword
MeSH Terms
Figure
-
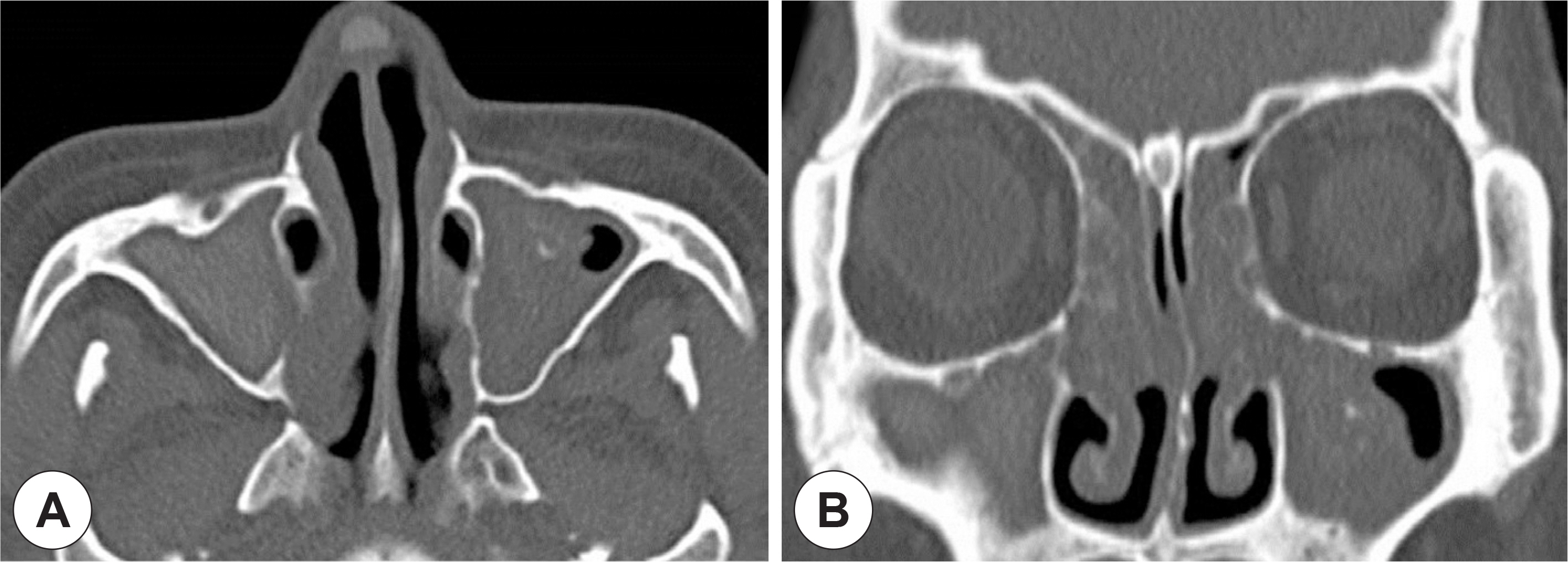
Fig. 1. Preoperative axial (A) and coronal (B) CT scan showing total opacifi-cation of both maxillary, ethmoid sinuses with hyperattenuation in central portion of right maxillary sinus and calcification in central area of left maxillary sinus.
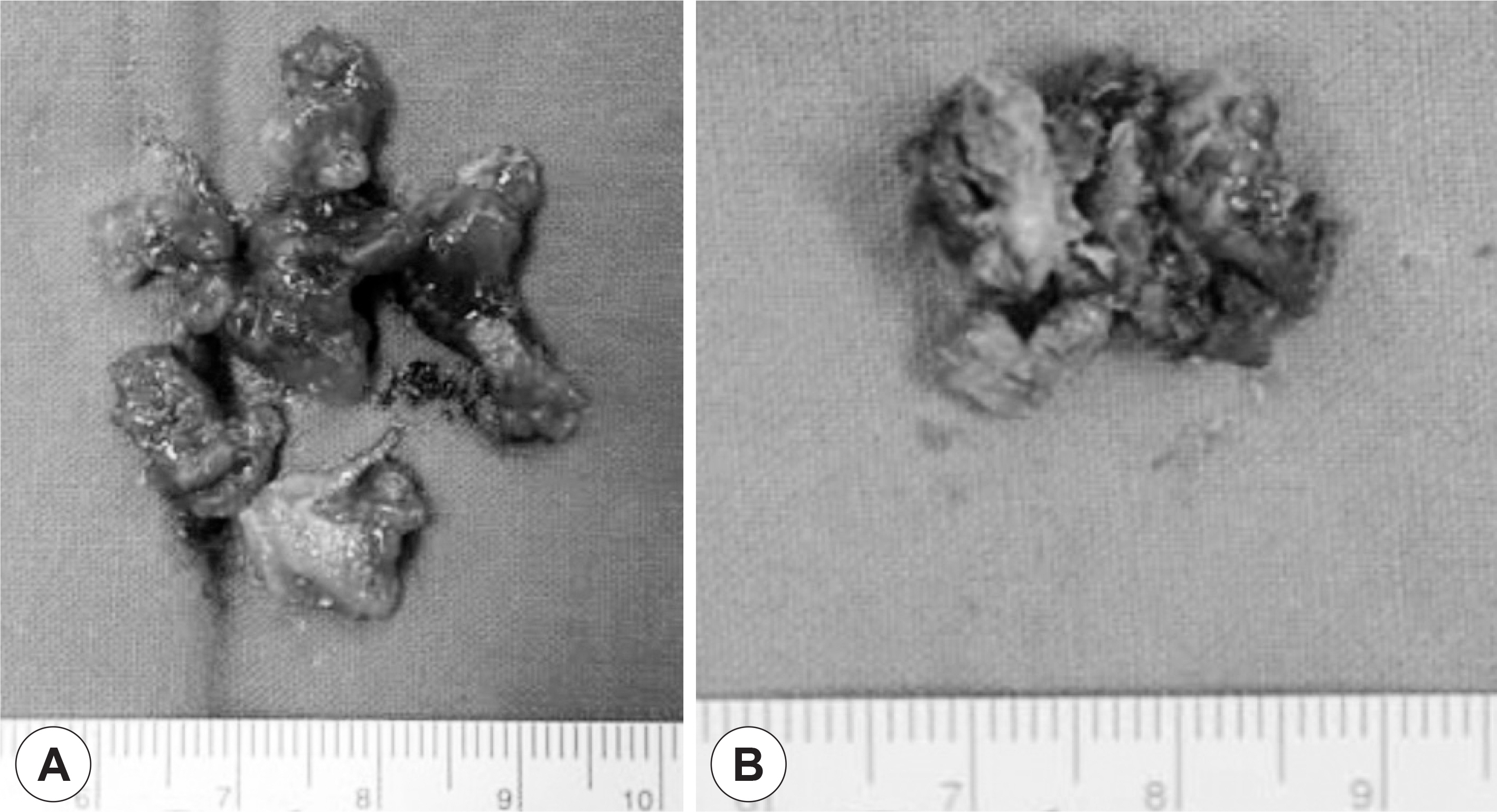
Fig. 2. Thick, inspissated greenish mucoid secretion was removed from right maxillary sinus (A). Dark brown-colored clay-like material was brought out from left maxillary sinus (B).

Fig. 3. H&E stain of right maxillary sinus lesion showing inflammatory cells composed predominantly eosinophils and Charcot-Leden crystals (A). GMS stain of right maxillary sinus lesion was positive for fungal hyphae (B). H&E stain of left maxillary sinus lesion showing aggregation of fungal hyphae, consistent with Aspergillosis (C).

Fig. 4. Six months after surgery, endoscopic findings of polypoid mucosa with yellowish thick discharge in right sphenoethmoidal recess (A). After use of systemic steroid therapy for one week (Prednisolone 20mg per day), both yellowish discharge and polypoid lesion disappeared (B).
Reference
-
References
1). McClay JE, Marple B, Kapadia L, Biavati MJ, Nussenbaum B, Newcomer M, et al. Clinical presentation of allergic fungal sinusitis in children. Laryngoscope. 2002; 112:565–9.
Article2). Marple BF. Allergic fungal rhinosinusitis: current theories and management strategies. Laryngoscope. 2001; 111:1006–19.
Article3). Nicolai P, Lombardi D, Tomenzoli D, Villaret AB, Piccioni M, Mensi M, et al. Fungus ball of the paranasal sinuses: experience in 160 patients treated with endoscopic surgery. Laryngoscope. 2009; 119:2275–9.
Article4). Dufour X, Kauffmann-Lacroix C, Ferrie JC, Goujon JM, Rodier MH, Karkas A, et al. Paranasal sinus fungus ball and surgery: a review of 175 cases. Rhinology. 2005; 43:34–9.5). Silva MP, Baroody FM. Allergic fungal rhinosinusitis. Ann Allergy Asthma Immunol. 2013; 110(4):217–22.
Article6). Manning SC, Holman M. Further evidence for allergic pathophysiology in allergic fungal sinusitis. Laryngoscope. 1998; 108:1485–96.
Article7). Bent JP 3rd, Kuhn FA. Diagnosis of allergic fungal sinusitis. Otolaryngol Head Neck Surg. 1994; 111:580–8.
Article8). Collins M, Nair S, Smith W, Kette F, Gillis D, Wormald PJ. Role of local immunoglobulin E production in the pathophysiology of non-invasive fungal sinusitis. Laryngoscope. 2004; 114(7):1242–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Characteristics and Treatment of Fungal Rhinosinusitis
- Non-surgical Management of Fungal Sinusitis
- A Case of Fungal Ball Caused by Retained Glass Foreign Body in Maxillary Sinus for 30 Years
- A Case of Allergic Mucin Sphenoiditis without Fungus
- Rhinolith Arising from Fungus Ball in the Nasal Cavity
