Coexistence of AA and AL Cardiac Amyloidosis in a Patient with Ankylosing Spondylitis Accompanying Monoclonal Gammopathy of Undetermined Significance
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. seungki73@catholic.ac.kr
- 2Department of Radiology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2297528
- DOI: http://doi.org/10.4078/jrd.2014.21.3.151
Abstract
- Amyloidosis is a clinical disorder caused by extracellular deposition of proteinaceous insoluble fibrils in various tissues, resulting in organ compromise. Amyloid L (AL) amyloidosis is the most common type of systemic amyloidosis, which occurs in association with multiple myeloma or monoclonal gammopathy of undetermined significance (MGUS). Secondary amyloid A (AA) amyloidosis is a complication of chronic inflammatory conditions, such as rheumatoid arthritis or ankylosing spondylitis. We report a case of a 49-year-old manwith a 11-year history of ankylosing spondylitis, who was recently diagnosed with MGUS presented with cardiac amyloidosis of both the AA and AL types. We report this case along with a review of relevant literature.
Keyword
MeSH Terms
Figure
-

Figure 1. Lumbar radiography shows squaring of the body with the syndesmophyte along the disc margin of the lumbar spine. Facet anklyosis of the lower lumbar spine.
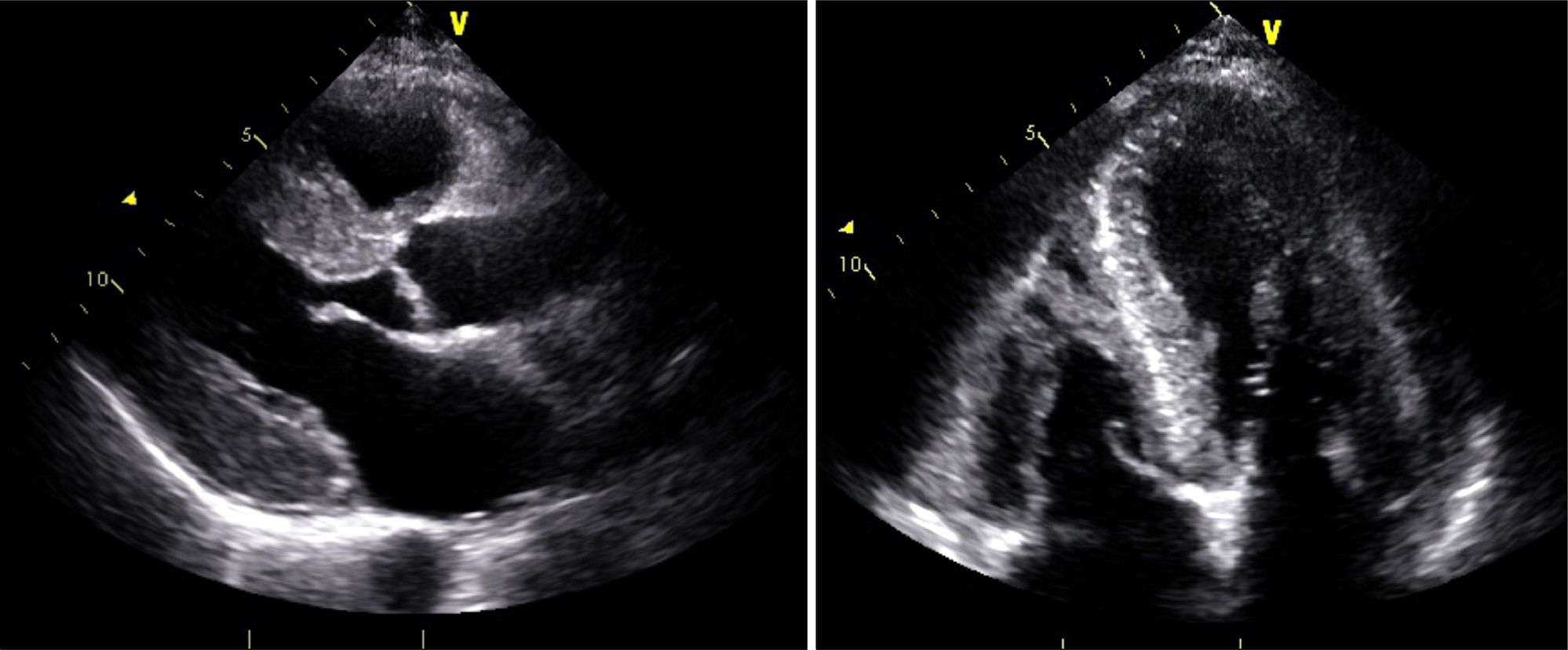
Figure 2. Echocardiography demonstrated a ground glass opacity pattern of the myocardium and increased wall thickness (septal thickness, 15.9 mm; posterior wall thickness, 14.4 mm).
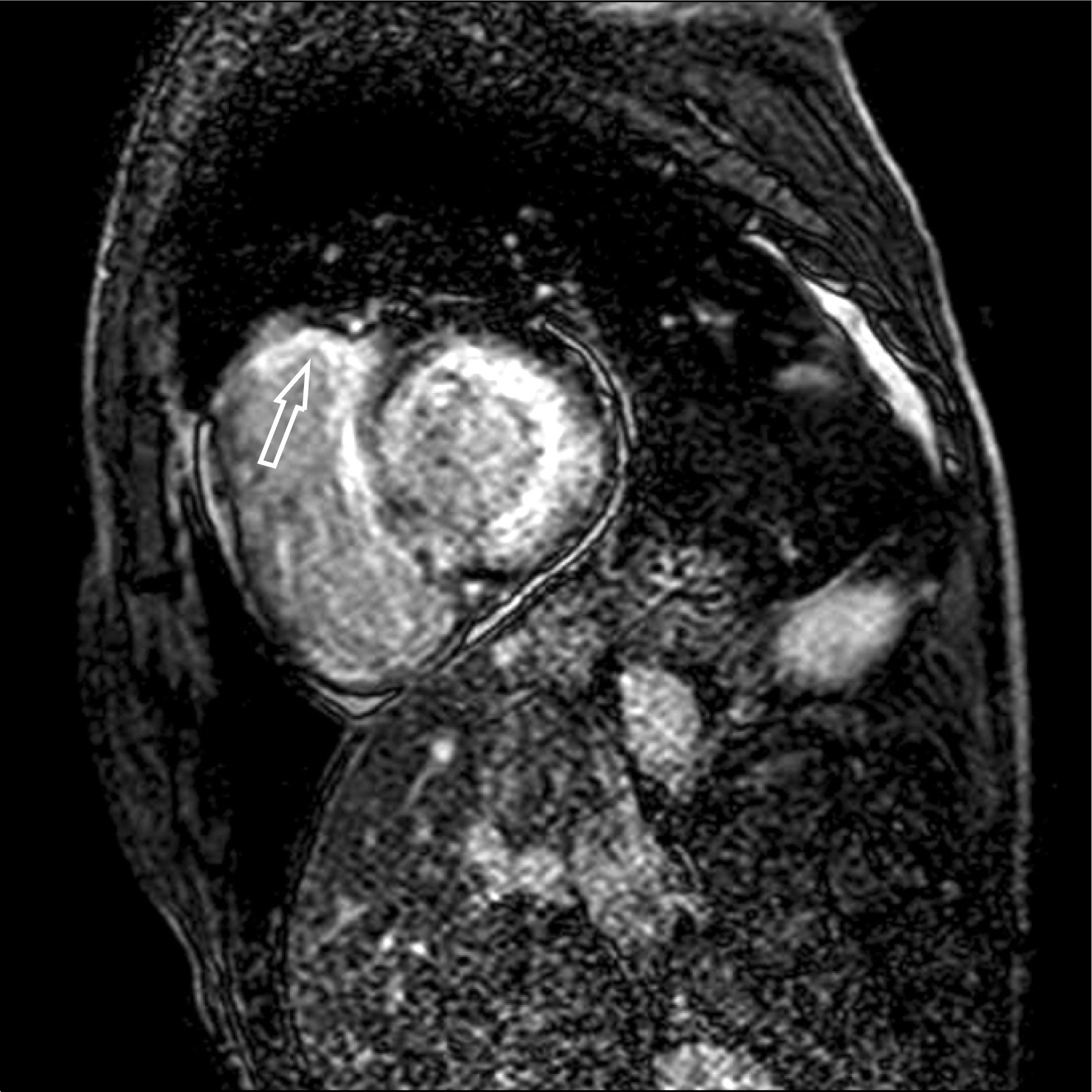
Figure 3. Midventricular short-axis LGE-CMR image shows global subendocardial LGE of the left ventricle and patchy transmural enhancement of right ventricle (arrow). LGE: late gadolinium enhancement, CMR: cardiac magnetic resonance.

Figure 4. Immunohistochemical staining of the heart biopsy showing amyloid A (AA) amyloidosis with amyloid L (AL) amylodosis. (A) AA protein (×200). (B) Lambda light chain (×200).

Figure 5. Electron microscope revealed interstitial deposition of amorphous material with thin fibrils, consistent with amyloidosis.
Reference
-
1. Cunnane G. Amyloid precursors and amyloidosis in inflammatory arthritis. Curr Opin Rheumatol. 2001; 13:67–73.
Article2. Husby G. Amyloidosis. Semin Arthritis Rheum. 1992; 22:67–82.
Article3. Desai HV, Aronow WS, Peterson SJ, Frishman WH. Cardiac amyloidosis: approaches to diagnosis and management. Cardiol Rev. 2010; 18:1–11.4. Wright JR, Calkins E, Humphrey RL. Potassium perman-ganate reaction in amyloidosis. A histologic method to assist in differentiating forms of this disease. Lab Invest. 1977; 36:274–81.5. Marhaug G, Dowton SB. Serum amyloid A: an acute phase apolipoprotein and precursor of AA amyloid. Baillieres Clin Rheumatol. 1994; 8:553–73.
Article6. Jung SY, Park MC, Park YB, Lee SK. Serum amyloid a as a useful indicator of disease activity in patients with ankylosing spondylitis. Yonsei Med J. 2007; 48:218–24.
Article7. Carroll JD, Gaasch WH, McAdam KP. Amyloid cardiomyopathy: characterization by a distinctive volt-age/mass relation. Am J Cardiol. 1982; 49:9–13.
Article8. Brown LM, Gridley G, Check D, Landgren O. Risk of multiple myeloma and monoclonal gammopathy of undetermined significance among white and black male United States veterans with prior autoimmune, infectious, inflammatory, and allergic disorders. Blood. 2008; 111:3388–94.
Article9. Perry ME, Stirling A, Hunter JA. Effect of etanercept on serum amyloid A protein (SAA) levels in patients with AA amyloidosis complicating inflammatory arthritis. Clin Rheumatol. 2008; 27:923–5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Concurrence of Fibrillary Glomerulonephritis and AL Amyloidosis Associated with Monoclonal Gammopathy
- The Association between Multiple Myeloma and Ankylosing Spondylitis: A Report of Two Cases
- Polyneuropathy Associated with IgA Paraproteinemia and Amyloidosis: A Case Report and Literature Review
- Monoclonal Gammopathy of Undetermined Significance Presented as a Vasculitic Neuropathy
- Cryoglobulinemia with a Digital Gangrene from Monoclonal Gammopathy of Undetermined Significance
