J Korean Ophthalmol Soc.
2016 Jun;57(6):999-1003. 10.3341/jkos.2016.57.6.999.
A Case of Staphylococcus lugdunensis Endophthalmitis after Cataract Surgery
- Affiliations
-
- 1Myunggok Eye Research Center, Department of Ophthalmology, Kim's Eye Hospital, Konyang University College of Medicine, Seoul, Korea. idoc@kimeye.com
- KMID: 2290506
- DOI: http://doi.org/10.3341/jkos.2016.57.6.999
Abstract
- PURPOSE
To report a case of Staphylococcus lugdunensis endophthalmitis following cataract extraction and intraocular lens implantation.
CASE SUMMARY
A 59-year-old woman presented with unilateral vision impairment and eyeball pain in her left eye, thirteen days after phacoemulsification and posterior chamber intraocular lens implantation. Best-corrected visual acuity of her left eye was 20/200. Slit lamp examination of her left eye revealed a severe conjunctival injection, severe chamber reactions with exudative membranes, hypopyon (about 1 mm) in the anterior chamber, and the fundus was not visible. Before the patient was admitted to the hospital, we cultured samples of aqueous fluid and performed an intravitreal antibiotics injection (vancomycin 1.0 mg/0.1 mL, ceftazidime 2.0 mg/0.1 mL). However, on the next day, because the inflammatory reactions of the anterior chamber and vitreous cavity were not improved and Gram positive cocci was confirmed, we performed a pars plana vitrectomy and an additional intravitreal antibiotics injection (vancomycin 1.0 mg/0.1 mL, dexamethasone 0.5 mg/0.1 mL). Seven days after the surgery, Staphylococcus lugdunensis was identified in the aqueous fluids culture. 11 days after the surgery, her inflammation and symptoms were improved and therefore, she could be discharged. Three months after the surgery, best-corrected visual acuity of her left eye was 20/20 and there was no evidence of recurrence of endophthalmitis and no abnormal findings in her fundus.
Keyword
MeSH Terms
-
Anterior Chamber
Anti-Bacterial Agents
Cataract Extraction
Cataract*
Ceftazidime
Dexamethasone
Endophthalmitis*
Female
Gram-Positive Cocci
Humans
Inflammation
Lens Implantation, Intraocular
Membranes
Middle Aged
Phacoemulsification
Recurrence
Slit Lamp
Staphylococcus lugdunensis*
Staphylococcus*
Visual Acuity
Vitrectomy
Anti-Bacterial Agents
Ceftazidime
Dexamethasone
Figure
-
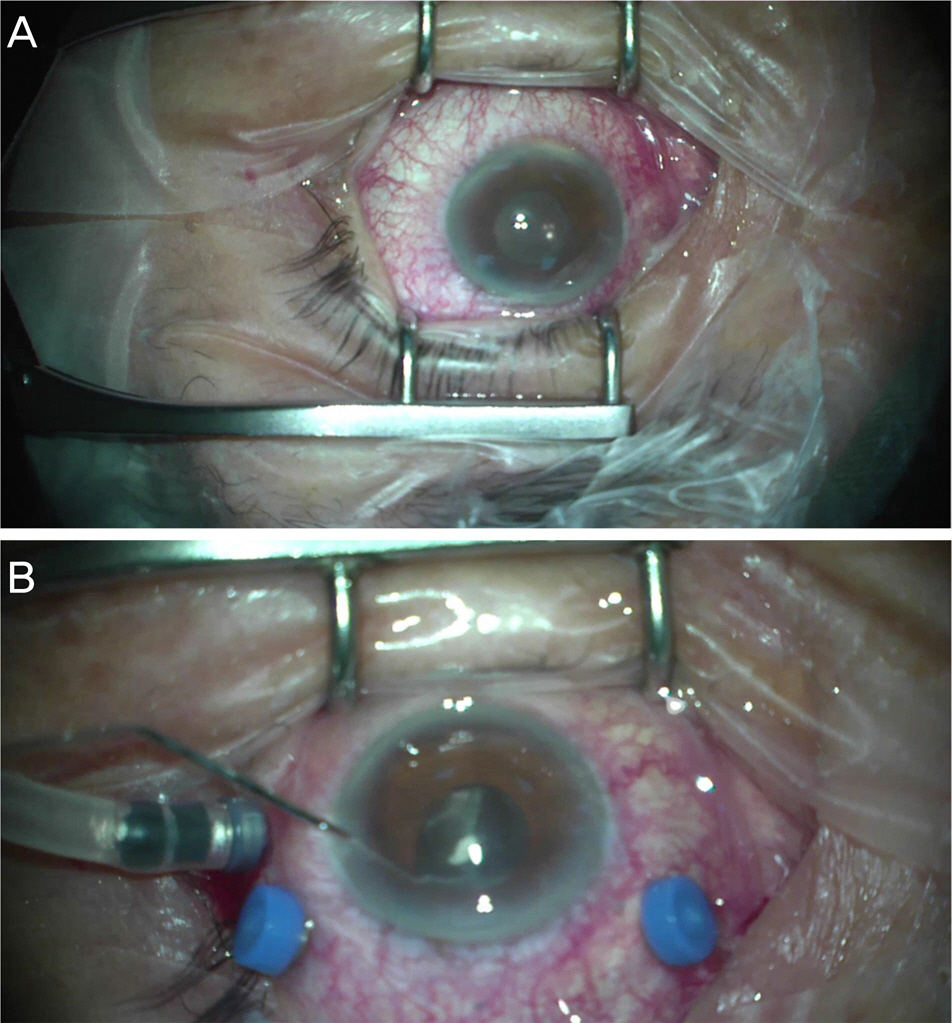
Figure 1. Pre- and intraoperative findings. (A) Just before vitrectomy, anterior segment shows severe conjunctival injection and hypopyon. (B) Thick, exudative membranes were found in anterior chamber.

Figure 2. Intraoperative fundus finding. At the end of vitrectomy, there was no inflammation or retinal hemorrhages on her left fundus.

Figure 3. Postoperative fundus finding. At 3 months after vitrectomy, there was no inflammation or infection signs on fundus photo.
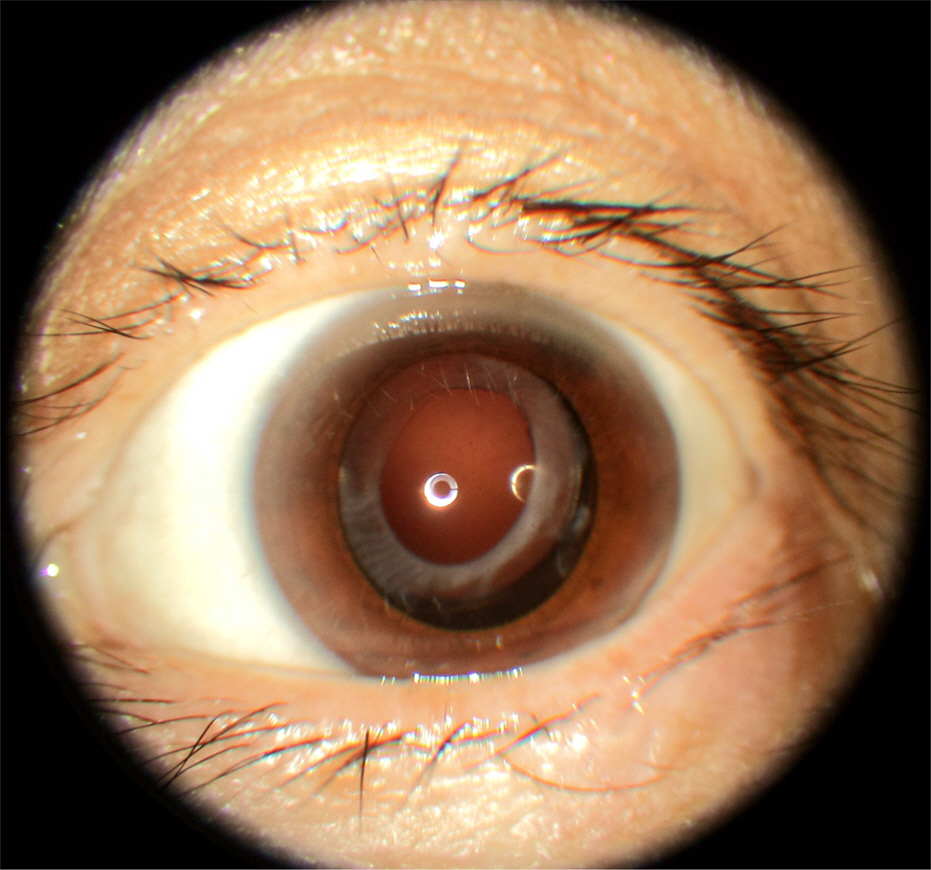
Figure 4. Anterior segment photography. Anterior segment photography on 3 months postoperative day shows clear cornea, normal anterior chamber, and posterior capsular intraocular lens was in place.
Reference
-
References
1. Lalwani GA, Flynn HW Jr, Scott IU, et al. Acute-onset endophthalmitis after clear corneal cataract surgery (1996–2005). Clinical features, causative organisms, and visual acuity outcomes. Ophthalmology. 2008; 115:473–6.2. Doft BH, Kelsey SF, Wisniewski S, et al. Treatment of endophthalmitis after cataract extraction. Retina. 1994; 14:297–304.
Article3. Laatikainen L, Tarkanen A. Early vitrectomy in the treatment of abdominal purulent endophthalmitis. Acta Ophthalmol (Copenh). 1987; 65:455–60.4. Jung JY, Ko BY, Kim BY. Factors associated with a poor visual result in acute endophthalmitis after cataract surgery. J Korean Ophthalmol Soc. 2008; 49:1242–7.
Article5. Han YS, Chung IY, Park JM. A case of Alcaligenes xylosoxidans endophthalmitis after cataract extraction. J Korean Ophthalmol Soc. 2005; 46:186–9.6. Bannerman TL, Rhoden DL, McAllister SK, et al. The source of coagulase-negative staphylococci in the Endophthalmitis Vitrectomy Study. A comprarison of eyelid and intraocular isolates using pulsed-field gel electrophoresis. Arch Ophthalmol. 1997; 115:357–61.7. Results of the Endophthalmitis Vitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Endophthalmitis Vitrectomy Study Group. Arch Ophthalmol. 1995; 113:1479–96.8. Han DP, Wisniewski SR, Wilson LA, et al. Spectrum and abdominal of microbiologic isolates in the Endophthalmitis Vitrectomy Study. Am J Ophthalmol. 1996; 122:1–17.9. Kunimoto DY, Das T, Sharma S, et al. Microbiologic spectrum and susceptibility of isolates: part I. postoperative endophthalmitis. Endophthalmitis Research Group. Am J Ophthalmol. 1999; 128:240–2.10. von Eiff C, Peters G, Heilmann C. Pathogenesis of infections due to coagulase-negative staphylococci. Lancet Infect Dis. 2002; 2:677–85.
Article11. Chiquet C, Pechinot A, Creuzot-Garcher C, et al. Acute abdominal endophthalmitis caused by Staphylococcus lugdunensis. J Clin Microbiol. 2007; 45:1673–8.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bilateral Staphylococcus Epidermidis Endophthalmitis After Cataract Extraction
- Bacterial Culture of conjuncitiva and Aqueous Humor in Cotaract Surgery
- A Case of Pulmonary Artery Endarteritis due to Staphylococcus lugdunensis in Patient with Clinically Silent Patent Ductus Arteriosus
- A Case of Psoas Abscess Caused by Staphylococcus lugdunensis
- A Case of Septicemia by Staphylococcus lugdunensis
