Ultrasonographic Evaluation of Flexor Hallucis Longus Tenosynovitis in Sports Players
- Affiliations
-
- 1KT Lee's Orthopedic Hospital, Seoul, Korea.
- 2Department of Orthopedics, Sun Genenral Hospital, Daejeon, Korea. kjb9290@hanmail.net
- KMID: 2288608
- DOI: http://doi.org/10.5763/kjsm.2013.31.2.51
Abstract
- The purpose of this study was to investigate the ultrasonographic features of flexor hallucis longus (FHL) tenosynovitis in sports players. High-resoluted ultrasound was used to measure the thickness and echogenicity of the flexor hallucis longus at the posteromedial ankle, especially the fibro-osseous tunnel, for 60 sports players (120 feet). They were compared with their asymptomatic feet. There were two group; group 1 was symptomatic feet, 2 was asymptomatic. The 36 males (72 feet) and 24 females (48 feet) had an average age of 21.3 years (range, 18.23 years). Thickness, echogenicity of the tendon on each group were evaluated by the ultrasonography and the results were statistically analyzed. The mean thickness of the FHL on group 1 was 3.4+/-1.2 mm, 2.1+/-1.3 mm on group 2. There was significant difference between two groups (p=0.002). The thickness of FHL based on gender and location was not significant different (p>0.05). For group 1, increased thickness of the FHL and reduced echogenicity, peritendious fluid collection were observed in ultrasonographic findings.Increased thickness (>3 mm) and hypoechoic lesion, peritendinous fluid collection of the tendon were sonographic findings at the posteromedial ankle in the FHL tenosynovitis. The authors suggested that Ultrasonography is a valuable and alternative tool for the evaluation of FHL tenosynovitis.
Keyword
MeSH Terms
Figure
-

Fig. 1. There is a ultrasonographic finding on longitudinal view, at the fibroosseous tunnel of the ankle. (A) The probe was located to the parallel of driving direction of the tendon. (B) The thickness and echogenicity of it was checked, on the ultrasonographic view.
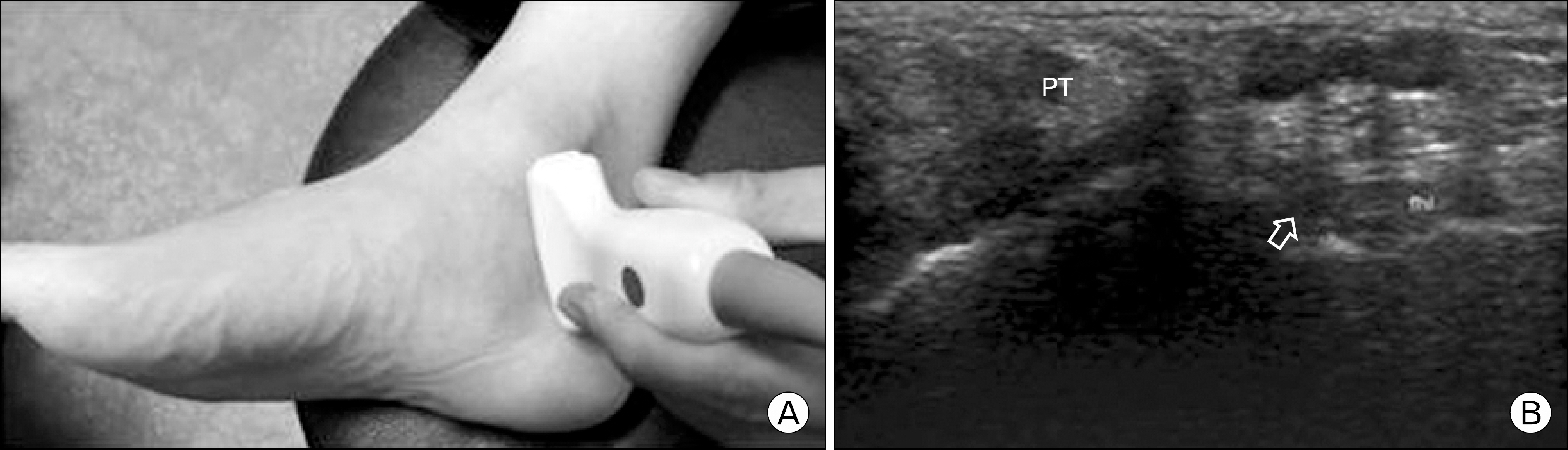
Fig. 2. There is a ultrasonographic finding on axial view, at the fibroosseous tunnel of the ankle. (A) The probe was located to the perpendicular of driving direction of the tendon. (B) The echogenicity of it was checked, on the ultrasonographic view. This shows the target sign (arrow). PT: posterior tibialis.
Cited by 1 articles
-
Diagnosis and Comorbidity of Chronic Ankle Instability
Dongjun Ha, Duckhee Kim, Heuichul Gwak
J Korean Foot Ankle Soc. 2018;22(2):49-54. doi: 10.14193/jkfas.2018.22.2.49.
Reference
-
References
1. Hamilton W, Chao W. Posterior ankle pain in athletes and dancers. Foot Ankle Clin. 1999; 4:811–32.2. Hardaker WT Jr, Margello S, Goldner JL. Foot and ankle injuries in theatrical dancers. Foot Ankle. 1985; 6:59–69.
Article3. Kolettis GJ, Micheli LJ, Klein JD. Release of the flexor hallucis longus tendon in ballet dancers. J Bone Joint Surg Am. 1996; 78:1386–90.
Article4. Leitschuh PH, Zimmerman JP, Uhorchak JM, Arciero RA, Bowser L. Hallux flexion deformity secondary to entrapment of the flexor hallucis longus tendon after fibular fracture. Foot Ankle Int. 1995; 16:232–5.
Article5. Khoury V, Guillin R, Dhanju J, Cardinal E. Ultrasound of ankle and foot: overuse and sports injuries. Semin Musculoskelet Radiol. 2007; 11:149–61.
Article6. Klauser A, Bodner G, Frauscher F, Gabl M, Zur Nedden D. Finger injuries in extreme rock climbers. Assessment of high-resolution ultrasonography. Am J Sports Med. 1999; 27:733–7.7. Torriani M, Kattapuram SV. Musculoskeletal ultrasound: an alternative imaging modality for sports-related injuries. Top Magn Reson Imaging. 2003; 14:103–11.
Article8. Michelson J, Dunn L. Tenosynovitis of the flexor hallucis longus: a clinical study of the spectrum of presentation and treatment. Foot Ankle Int. 2005; 26:291–303.
Article9. Hamilton WG. Stenosing tenosynovitis of the flexor hallucis longus tendon and posterior impingement upon the os trigo-num in ballet dancers. Foot Ankle. 1982; 3:74–80.
Article10. McCarroll JR, Ritter MA, Becker TE. Triggering of the great toe. A case report. Clin Orthop Relat Res. 1983; 175:184–5.11. Sammarco GJ, Cooper PS. Flexor hallucis longus tendon injury in dancers and nondancers. Foot Ankle Int. 1998; 19:356–62.
Article12. Theodore GH, Kolettis GJ, Micheli LJ. Tenosynovitis of the flexor hallucis longus in a long-distance runner. Med Sci Sports Exerc. 1996; 28:277–9.
Article13. Petersen W, Pufe T, Zantop T, Paulsen F. Blood supply of the flexor hallucis longus tendon with regard to dancer's ten-dinitis: injection and immunohistochemical studies of cadaver tendons. Foot Ankle Int. 2003; 24:591–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Trigger Toe in Soccer Player: A Case Report
- Clinical Outcomes and Complications of Tendoscopic Treatment for Flexor Hallucis Longus Tenosynovitis
- The Checkrein Deformity of Extensor Hallucis Longus Tendon and Extensor Retinaculum Syndrome with Deep Peroneal Nerve Entrapment after Triplane Fracture: A Case Report
- Tendonitis of the Flexor Hallucis Longus with Triggering of the Great Toe: A Case Report
- Proximal Flexor Hallucis Longus Tendon Transfer for the Ossification of the Achilles Tendon: A Case Report
