J Breast Cancer.
2011 Jun;14(2):119-123. 10.4048/jbc.2011.14.2.119.
Ultrasound and Clinicopathological Characteristics of Triple Receptor-Negative Breast Cancers
- Affiliations
-
- 1Department of Radiology, Breast and Thyroid Cancer Center, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. yoonchoi99@gmail.com
- 2Department of Radiology, Dream Hospital, Daegu, Korea.
- 3Department of Surgery, Breast and Thyroid Cancer Center, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2286510
- DOI: http://doi.org/10.4048/jbc.2011.14.2.119
Abstract
- PURPOSE
Triple receptor-negative (TRN) breast cancer is associated with high risk of recurrence and poor prognosis. The present study assessed the clinicopathologic characteristics and ultrasound (US) features of TRN breast cancers.
METHODS
Pathological and biological data were reviewed for 558 breast cancer patients treated at Kangbuk Samsung Hospital, between January 2003 and December 2009. The patients were separated into TRN breast cancer and non-TRN breast cancer groups, based on the results of immunohistochemical prognostic panels. Clinical and pathologic features were compared for the two groups. US features, including shape, orientation, margins, boundaries, echo patterns, posterior acoustic features, surrounding tissues, and microcalcifications, were determined for 41 TRN patients and 189 non-TRN controls (ER+/PR+/HER2-).
RESULTS
Of 558 cases, 58 (10.4%) had the TRN phenotype. Four hundred and thirty-four cases (77.8%) were invasive ductal carcinomas. TRN cancer was significantly associated with specific characteristics of tumor size, nuclear grade, histologic grade, venous invasion, and lymphatic invasion. With respect to US features, TRN cancers were more likely to have an oval shape, a circumscribed margin, and marked hypoechogenicity.
CONCLUSION
Tumor characteristics were different between TRN and non-TRN breast cancers, although US cannot differentiate the subtype of breast cancers TRN cancer tend to show somewhat different US morphology.
Keyword
MeSH Terms
Figure
-
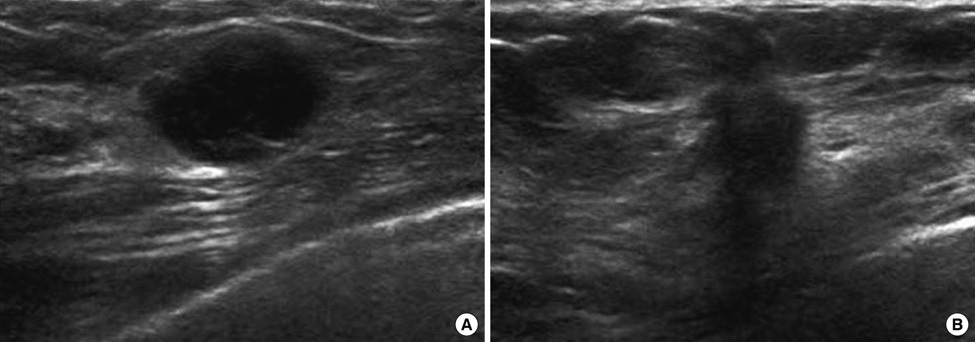
Figure 1 Ultrasonographic findings. (A) The image of a triple receptor-negative invasive ductal carcinoma in a 30-year-old-woman. It shows an oval shaped and well circumscribed markedly hypoechoic mass without posterior shadowing. (B) The image of a non-TRN (ER+/PR+/HER2-) invasive ductal carcinoma in a 47-year-old-woman. It shows irregular shaped hypoechoic mass with spiculated margin and posterior shadowing.
Reference
-
1. Akiyama F, Iwase H. Triple negative breast cancer: clinicopathological characteristics and treatment strategies. Breast Cancer. 2009. 16:252–253.
Article2. Bauer KR, Brown M, Cress RD, Parise CA, Caggiano V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: a population-based study from the California cancer Registry. Cancer. 2007. 109:1721–1728.
Article3. Rakha EA, Ellis IO. Triple-negative/basal-like breast cancer: review. Pathology. 2009. 41:40–47.
Article4. Sasaki Y, Tsuda H. Clinicopathological characteristics of triple-negative breast cancers. Breast Cancer. 2009. 16:254–259.
Article5. Elias AD. Triple-negative breast cancer: a short review. Am J Clin Oncol. 2010. 33:637–645.6. Heitz F, Harter P, Lueck HJ, Fissler-Eckhoff A, Lorenz-Salehi F, Scheil-Bertram S, et al. Triple-negative and HER2-overexpressing breast cancers exhibit an elevated risk and an earlier occurrence of cerebral metastases. Eur J Cancer. 2009. 45:2792–2798.
Article7. Carey LA, Dees EC, Sawyer L, Gatti L, Moore DT, Collichio F, et al. The triple negative paradox: primary tumor chemosensitivity of breast cancer subtypes. Clin Cancer Res. 2007. 13:2329–2334.
Article8. Tian XS, Cong MH, Zhou WH, Zhu J, Chen YZ, Liu Q. Clinicopathologic and prognostic characteristics of triple-negative breast cancer. Onkologie. 2008. 31:610–614.
Article9. Rakha EA, El-Sayed ME, Green AR, Lee AH, Robertson JF, Ellis IO. Prognostic markers in triple-negative breast cancer. Cancer. 2007. 109:25–32.
Article10. Grann VR, Troxel AB, Zojwalla NJ, Jacobson JS, Hershman D, Neugut AI. Hormone receptor status and survival in a population-based cohort of patients with breast carcinoma. Cancer. 2005. 103:2241–2251.
Article11. Carey LA, Perou CM, Livasy CA, Dressler LG, Cowan D, Conway K, et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA. 2006. 295:2492–2502.
Article12. Tan GH, Taib NA, Choo WY, Teo SH, Yip CH. Clinical characteristics of triple-negative breast cancer: experience in an Asian developing country. Asian Pac J Cancer Prev. 2009. 10:395–398.13. Ahn SH, Hwang UK, Kwak BS, Yoon HS, Ku BK, Kang HJ, et al. Prevalence of BRCA1 and BRCA2 mutations in Korean breast cancer patients. J Korean Med Sci. 2004. 19:269–274.
Article14. Ahn SH, Son BH, Kim SW, Kim SI, Jeong J, Ko SS, et al. Poor outcome of hormone receptor-positive breast cancer at very young age is due to tamoxifen resistance: nationwide survival data in Korea: a report from the Korean Breast Cancer Society. J Clin Oncol. 2007. 25:2360–2368.
Article15. Yoo KY, Kang D, Park SK, Kim SU, Kim SU, Shin A, et al. Epidemiology of breast cancer in Korea: occurrence, high-risk groups, and prevention. J Korean Med Sci. 2002. 17:1–6.
Article16. Seo BK, Pisano ED, Kuzimak CM, Koomen M, Pavic D, Lee Y, et al. Correlation of HER-2/neu overexpression with mammography and age distribution in primary breast carcinomas. Acad Radiol. 2006. 13:1211–1218.
Article17. Yang WT, Dryden M, Broglio K, Gilcrease M, Dawood S, Dempsey PJ, et al. Mammographic features of triple receptor-negative primary breast cancers in young premenopausal women. Breast Cancer Res Treat. 2008. 111:405–410.
Article18. Wang Y, Ikeda DM, Narasimhan B, Longacre TA, Bleicher RJ, Pal S, et al. Estrogen receptor-negative invasive breast cancer: imaging features of tumors with and without human epidermal growth factor receptor type 2 overexpression. Radiology. 2008. 246:367–375.
Article19. Ko ES, Lee BH, Kim HA, Noh WC, Kim MS, Lee SA. Triple-negative breast cancer: correlation between imaging and pathological findings. Eur Radiol. 2010. 20:1111–1117.
Article20. Karamouzis MV, Likaki-Karatza E, Ravazoula P, Badra FA, Koukouras D, Tzorakoleftherakis E, et al. Non-palpable breast carcinomas: correlation of mammographically detected malignant-appearing microcalcifications and molecular prognostic factors. Int J Cancer. 2002. 102:86–90.
Article21. Field AS, Chamberlain NL, Tran D, Morey AL. Suggestions for HER-2/neu testing in breast carcinoma, based on a comparison of immunohistochemistry and fluorescence in situ hybridisation. Pathology. 2001. 33:278–282.
Article22. Yaziji H, Goldstein LC, Barry TS, Werling R, Hwang H, Ellis GK, et al. HER-2 testing in breast cancer using parallel tissue-based methods. JAMA. 2004. 291:1972–1977.
Article23. Yaziji H, Gown AM. Testing for epidermal growth factor receptor in lung cancer: have we learned anything from HER-2 testing? J Clin Oncol. 2004. 22:3646.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- MRI Findings of Triple Negative Breast Cancer: A Comparison with Non-Triple Negative Breast Cancer
- Clinicopathologic Characteristics and Prognosis of Early Stage Triple Negative Breast Cancer: Comparison with Non-triple Negative Group
- Imaging Surveillance for Survivors of Breast Cancer: Correlation between Cancer Characteristics and Method of Detection
- The nature of triple-negative breast cancer classification and antitumoral strategies
- Hereditary Breast Cancer in Korea: A Review of the Literature
