Cervical Lymphadenitis Caused by Group D Non-typhoidal Salmonella Associated with Concomitant Lymphoma
- Affiliations
-
- 1Department of Internal Medicine, Dongnam Institution of Radiological and Medical Sciences, Busan, Korea.
- 2Division of Infectious Diseases, Department of Internal Medicine, Sungkyunkwan University School of Medicine, Seoul, Korea. collacin@hotmail.com
- 3Department of Laboratory Medicine and Genetics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Division of Hematology-Oncology, Department of Internal Medicine, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2285006
- DOI: http://doi.org/10.3947/ic.2013.45.2.234
Abstract
- Non-typhoidal Salmonella species are important foodborne pathogens that can cause gastroenteritis, bacteremia, and subsequent focal infections. Non-typhoidal salmonellosis is problematic, particularly in immunocompromised hosts. Any anatomical site can be affected by this pathogen via hematogenous seeding and may develop local infections. However, cervical lymphadenitis caused by non-typhoidal Salmonella species is rarely reported. Herein, we have reported a case of cervical lymphadenitis caused by group D non-typhoidal Salmonella associated with lymphoma.
Keyword
MeSH Terms
Figure
-

Figure 1 (A) The chest computed tomography scan shows an enlarged lymph node with necrosis in the right supraclavicular area and enhancement of the surrounding area. (B) The chest computed tomography scan shows a mass in the anterior mediastinum with necrosis that runs continuously from the supraclavicular area to the anterior mediastinum.
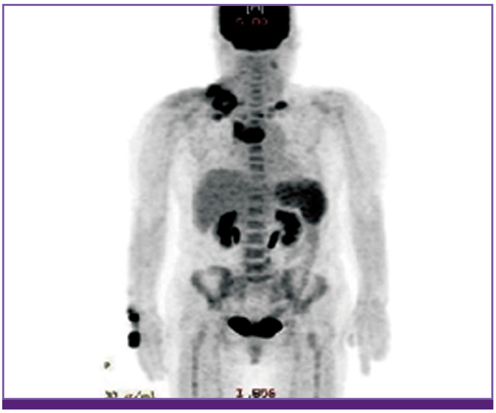
Figure 2 PET-torso image shows increased SUVmax of the lymph nodes in both the supraclavicular areas and anterior mediastinum.
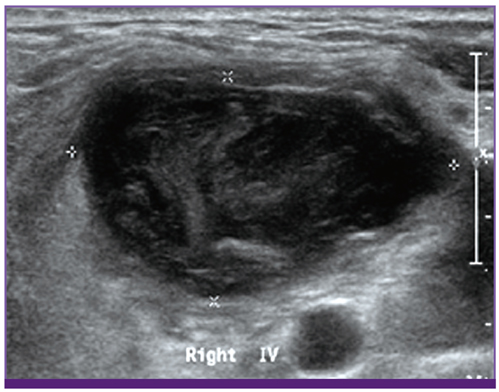
Figure 3 Ultrasonography image shows a lymph node in the right supraclavicular area (diameter is measured to 4 cm and minor axis is 2 cm), filled with debris and fluid.
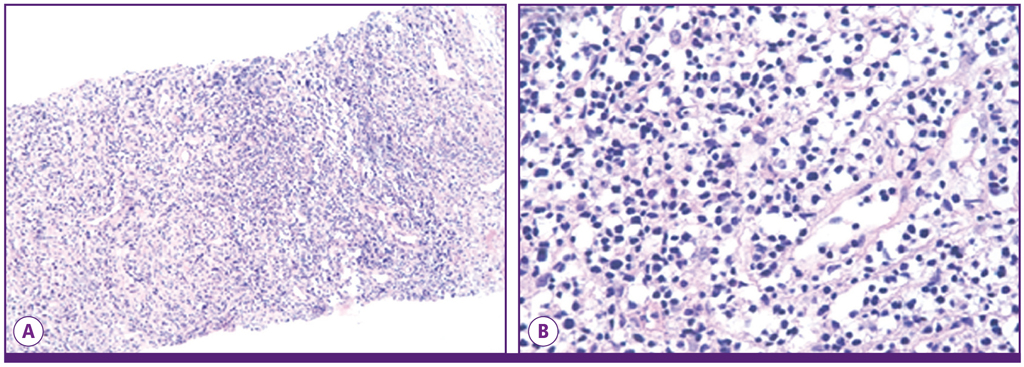
Figure 4 Histopathology of the cervical lymph node shows infarction and granulation tissue with focal lymphoid cells. (A) (hematoxylin and eosin [H&E] stain, ×100), (B) High magnification (hematoxylin and eosin [H&E] stain, ×400).
Reference
-
1. Chen PL, Chang CM, Wu CJ, Ko NY, Lee NY, Lee HC, Shih HI, Lee CC, Wang RR, Ko WC. Extraintestinal focal infections in adults with nontyphoid Salmonella bacteraemia: predisposing factors and clinical outcome. J Intern Med. 2007. 261:91–100.
Article2. Hohmann EL. Nontyphoidal salmonellosis. Clin Infect Dis. 2001. 32:263–269.
Article3. Campbell WN. Salmonella lymphadenitis associated with undiagnosed lymphoma. Eur J Clin Microbiol Infect Dis. 2001. 20:359–361.4. Peugues DA, Miller SI. Mandell GL, Bennett JE, Dolin R, editors. Salmonella species, including Salmonella typhi. Principles and Practice of Infectious Diseases. 2009. 7th ed. Philadelphia: Elsevier Churchill Livingstone;chapter 223.5. Cornut P, Courtieu AL. Suppurated cervical adenitis caused by Salmonella Typhi murium. Pediatrie. 1960. 15:169–173.6. García-Corbeira P, Ramos JM, Aguado JM, Soriano F. Six cases in which mesenteric lymphadenitis due to non-typhi Salmonella caused an appendicitis-like syndrome. Clin Infect Dis. 1995. 21:231–232.
Article7. Guarga A, Urrutia A, Paret A, Rey-Joly C. Mesenteric lymphadenitis caused by Salmonella Enteritidis. Med Clin (Barc). 1984. 82:136.8. Mautner LS, McIntyre AJ, Ord JV. Isolation of Salmonella organisms from mesenteric lymph nodes. Can Med Assoc J. 1961. 85:139–141.9. Meng GR. Acute mesenteric lymphadenitis due to Salmonella enteritidis mimicking appendicitis: case report. Mil Med. 1974. 139:277.
Article10. Murray JC, Singh RR, Brandt ML, Kearney DL, Ogden AK. Granulomatous submandibular lymphadenitis caused by Salmonella species in a healthy child. Clin Infect Dis. 1994. 19:1175–1176.
Article11. van de Vosse E, Ottenhoff TH, de Paus RA, Verhard EM, de Boer T, van Dissel JT, Kuijpers TW. Mycobacterium bovis BCG-itis and cervical lymphadenitis due to Salmonella enteritidis in a patient with complete interleukin-12/-23 receptor beta1 deficiency. Infection. 2010. 38:128–130.
Article12. Cohen JI, Bartlett JA, Corey GR. Extra-intestinal manifestations of Salmonella infections. Medicine (Baltimore). 1987. 66:349–388.13. Lee JH, Rhee PL, Lee JK, Lee KT, Son HJ, Kim JJ, Koh KC, Paik SW, Lee WJ, Lim HK, Rhee JC. The etiology and clinical characteristics of mesenteric adenitis in Korean adults. J Korean Med Sci. 1997. 12:105–110.
Article14. Likitnukul S, Wongsawat J, Nunthapisud P. Appendicitis-like syndrome owing to mesenteric adenitis caused by Salmonella typhi. Ann Trop Paediatr. 2002. 22:97–99.
Article15. Faber LM, Simoons-Smith AM, Razenberg PP. An unusual late manifestation of a Salmonella typhi infection. Am J Gastroenterol. 1990. 85:81–83.16. Singh NP, Manchanda V, Gomber S, Kothari A, Talwar V. Typhoidal focal suppurative lymphatic abscess. Ann Trop Paediatr. 2002. 22:183–186.
Article17. Lee S, Lee HN, Yang H, Kang J, Kim N, Sin Y, Lee S. A case of septic arthritis of the knee joint due to Group D non-typhoidal Salmonella. Infect Chemother. 2012. 44:303–306.
Article18. Cho KJ, Kim CW, Park SH, Lee SK. Necrotizing lymphadenitis-a clinico-pathologic study of 36 cases with immunohistochemical analysis. J Korean Med Sci. 1991. 6:55–61.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of an Infected Pseudoaneurysm with Complications Due to A Non-Typhoidal Salmonella Species
- The Serogroup and Antimicrobial Resistance of Salmonella spp. Isolated from the Clinical Specimens During 6 years in a Tertiary University Hospital
- A Case of Transverse Colon Perforation after Colonoscopy in a Patient withEnterocolitis Caused by Non-typhoidal Group D Salmonella
- A Case of Gallbladder Perforation Complicated by Acalculous Cholecystitis due to Non-Typhoidal Salmonella
- A Case of Septic Arthritis of the Knee Joint due to Group D Non-typhoidal Salmonella
