Correction of positional change of frontal cephalometric landmarks caused by vertical head rotation
- Affiliations
-
- 1Department of Orthodontics, 2nd Stage of Brain Korea 21, Dental Science Research Institute, School of Dentistry, Chonnam National University, Korea. hhwang@chonnam.ac.kr
- KMID: 2274246
- DOI: http://doi.org/10.4041/kjod.2011.41.2.98
Abstract
OBJECTIVE
Superimposition of frontal cephalograms cannot be performed when the cephalograms are taken with different vertical head rotations. The purpose of the present study was to evaluate the validity of correcting the positional change of frontal cephalometric landmarks caused by vertical head rotation.
METHODS
In 30 adult individuals, frontal and lateral cephalograms were taken at a 90degrees angle. Geometric principles of radiography were used to calculate the possible vertical and horizontal landmark changes if the head should be rotated down 5degrees about an ear rod axis. The calculated changes were then compared with cephalometric changes measured on frontal cephalogram actually taken with the head rotated down 5degrees.
RESULTS
When the frontal cephalograms were taken with the head rotated down 5degrees about an ear rod axis, significant changes in the vertical position of the landmarks occurred, particularly in the landmarks located farther anteriorly from the ear rod axis. The comparison of calculated changes and real cephalometric changes showed that the differences were less than 0.4 mm in the vertical direction and less than 0.2 mm in the horizontal direction. The differences between calculated and real changes were smaller in the landmarks less affected by vertical head rotation.
CONCLUSIONS
Even when frontal cephalograms are taken at different vertical head rotations, the concomitant changes in the position of the landmarks can be corrected through calculation using the geometric principle of radiography as long as frontal and lateral cephalograms are taken perpendicular to each other.
MeSH Terms
Figure
-

Fig. 1 The modified Head Posture Aligner used in this study.

Fig. 2 A, Frontal and lateral cephalograms were taken without head rotation using biplanar radiography; B, an additional frontal cephalogram was taken with the head rotated 5° down from the ear rod axis.

Fig. 3 The horizontal reference line on frontal cephalogram was defined as a line passing through the two ear rod ball markers, and the vertical reference line as a perpendicular line passing mid-point of the length of the horizontal reference line. The horizontal reference line on lateral cephalogram was established by drawing a line parallel to the horizontal wire incorporated in the Head Posture Aligner and passing through the ear rod ball marker, and the vertical reference line as a perpendicular line passing through the ear rod ball marker.
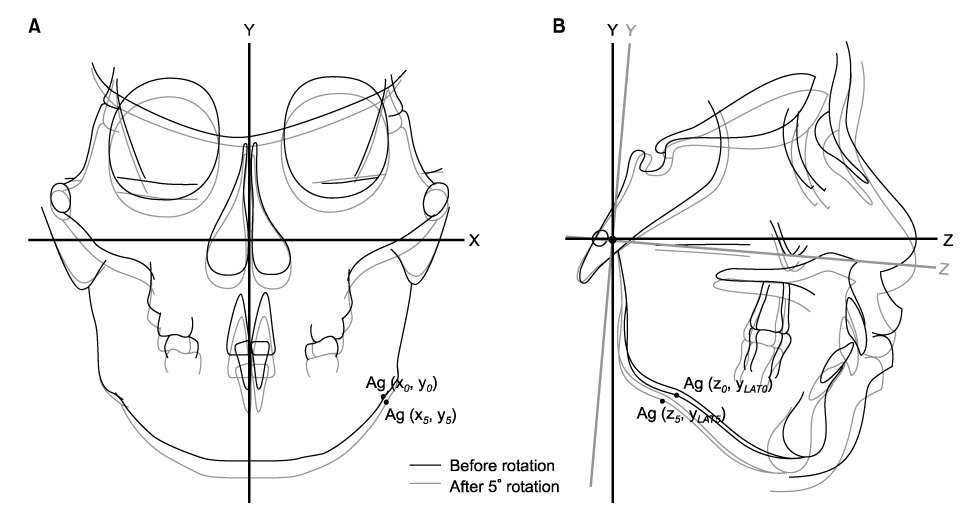
Fig. 4 Simulation of positional change of a landmark before and after a 5° downward head rotation and represented using an x, y coordinate system. Antegonion is used as an example. A, Frontal cephalometric tracings before and after head rotation; B, lateral cephalometric tracings before and after head rotation.
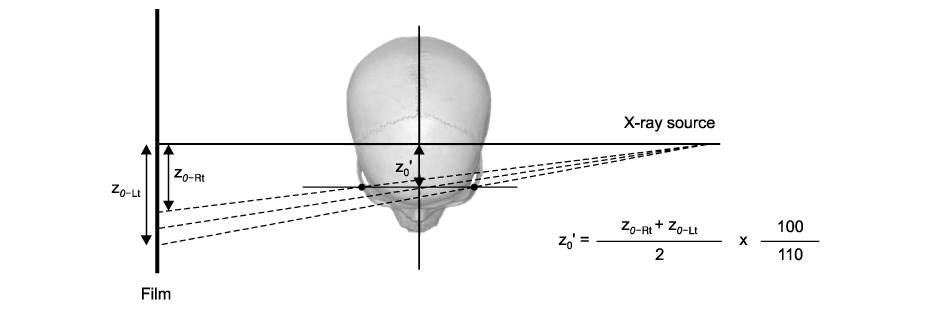
Fig. 5 Method of calculating z0' from lateral cephalogram. z0' is the actual horizontal distance from the ear rod axis to midpoint between right and left antegonions. z0-Rt is the horizontal position of right antegonion and z0-Lt is the horizontal position of left antegonion on lateral cephalogram.

Fig. 6 Schematic representation of radiographic magnification. Magnification of frontal cephalogram can be calculated using the lateral cephalogram, and magnification of lateral cephalogram can be calculated using the frontal cephalogram.
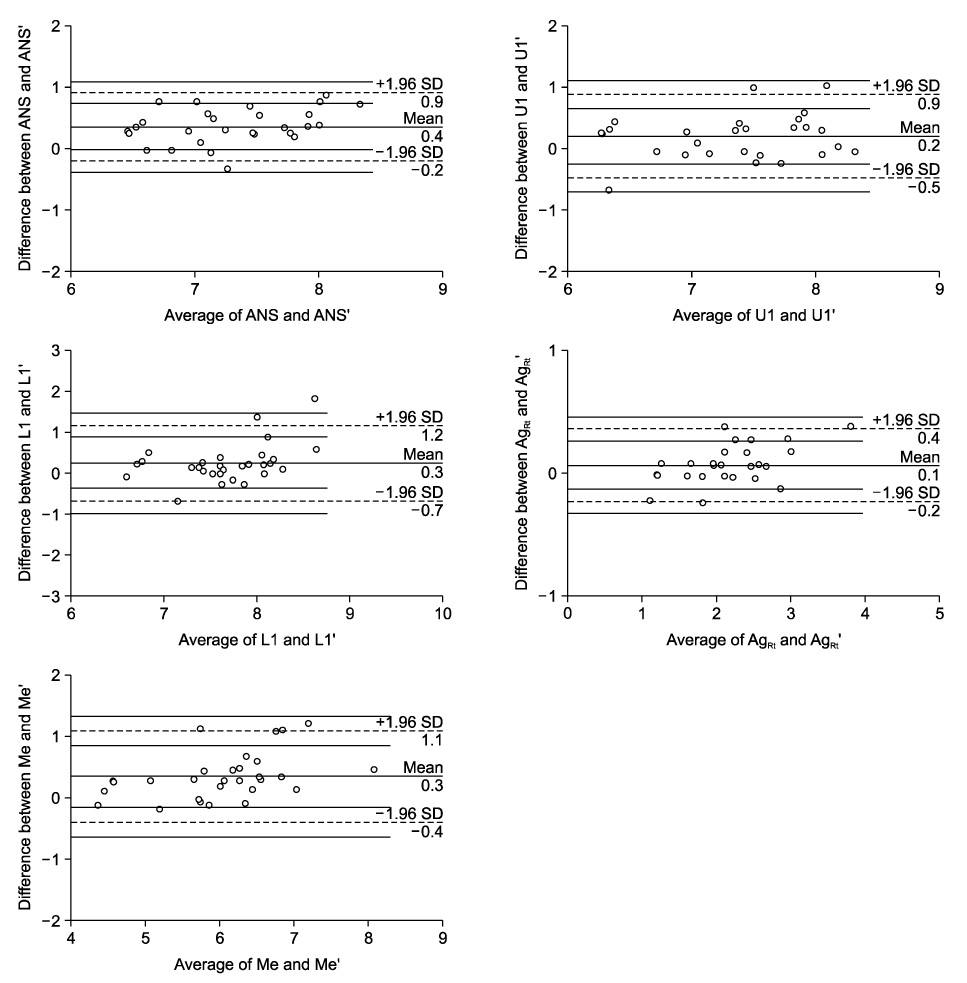
Fig. 7 Bland-Altman plots for variables ANS, U1, L1, AgRt, and Me in the vertical direction. The x-axis shows the average of the calculated and cephalometric changes, whereas the y-axis represents the difference between the two measurements. The limits of agreement are indicated by horizontal lines.
Reference
-
1. Broadbent BH. A new X-ray technique and its application to orthodontia. Angle Orthod. 1931. 1:45–66.2. Koh EH, Lee KH, Hwang HS. Effects of vertical head rotation on the posteroanterior cephalometric measurements. Korean J Orthod. 2003. 33:73–84.3. Proffit WR. Proffit WR, White RP, editors. The search for truth: diagnosis. Surgical orthodontic treatment. 1991. St. Louis: Mosby-Year Book;96–141.4. Kim EH, Hwang HS. The validity of Head Posture Aligner in posteroanterior cephaiometry. Korean J Orthod. 2000. 30:543–552.5. Cooke MS, Wei SH. An improved method for the assessment of the sagittal skeletal pattern and its correlation to previous methods. Eur J Orthod. 1988. 10:122–127.
Article6. Solow B, Tallgren A. Natural head position in standing subjects. Acta Odontol Scand. 1971. 29:591–607.
Article7. Solow B, Tallgren A. Head posture and craniofacial morphology. Am J Phys Anthropol. 1976. 44:417–435.
Article8. Solow B, Tallgren A. Dentoalveolar morphology in relation to craniocervical posture. Angle Orthod. 1977. 47:157–164.9. Solow B, Siersbaek-Nielsen S. Growth changes in head posture related to craniofacial development. Am J Orthod. 1986. 89:132–140.
Article10. Cooke MS, Wei SH. The reproducibility of natural head posture: a methodological study. Am J Orthod Dentofacial Orthop. 1988. 93:280–288.
Article11. Cooke MS. Five-year reproducibility of natural head posture: a longitudinal study. Am J Orthod Dentofacial Orthop. 1990. 97:489–494.
Article12. Peng L, Cooke MS. Fifteen-year reproducibility of natural head posture: A longitudinal study. Am J Orthod Dentofacial Orthop. 1999. 116:82–85.
Article13. Wenzel A, Williams S, Ritzau M. Relationships of changes in craniofacial morphology, head posture, and nasopharyngeal airway size following mandibular osteotomy. Am J Orthod Dentofacial Orthop. 1989. 96:138–143.
Article14. Achilleos S, Krogstad O, Lyberg T. Surgical mandibular setback and changes in uvuloglossopharyngeal morphology and head posture: a short- and long-term cephalometric study in males. Eur J Orthod. 2000. 22:383–394.
Article15. Tecco S, Festa F, Tete S, Longhi V, D'Attilio M. Changes in head posture after rapid maxillary expansion in mouth-breathing girls: a controlled study. Angle Orthod. 2005. 75:171–176.16. McGuinness NJ, McDonald JP. Changes in natural head position observed immediately and one year after rapid maxillary expansion. Eur J Orthod. 2006. 28:126–134.
Article17. Kusnoto B, Evans CA, BeGole EA, de Rijk W. Assessment of 3-dimensional computer-generated cephalometric measurements. Am J Orthod Dentofacial Orthop. 1999. 116:390–399.
Article18. Brown T, Abbott AH. Computer-assisted location of reference points in three dimensions for radiographic cephalometry. Am J Orthod Dentofacial Orthop. 1989. 95:490–498.
Article19. Eliasson S, Welander U, Ahlqvist J. The cephalographic projection. Part I: General considerations. Dentomaxillofac Radiol. 1982. 11:117–122.20. Ahlqvist J, Eliasson S, Welander U. The cephalometric projection. Part II. Principles of image distortion in cephalography. Dentomaxillofac Radiol. 1983. 12:101–108.21. Ahlqvist J, Eliasson S, Welander U. The effect of projection errors on cephalometric length measurements. Eur J Orthod. 1986. 8:141–148.
Article22. Hsiao TH, Chang HP, Liu KM. A method of magnification correction for posteroanterior radiographic cephalometry. Angle Orthod. 1997. 67:137–142.23. Major PW, Johnson DE, Hesse KL, Glover KE. Landmark identification error in posterior anterior cephalometrics. Angle Orthod. 1994. 64:447–454.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A comparative study of guiding methods for natural head posture in cephalometrics
- Changes of lateral cephalometric values according to the rotation of head
- Three dimensional analysis of maxillofacial structure by frontal and lateral cephalogram
- Positional Nystagmus Caused by Ketamine in Rabbits
- Effects of vertical head rotation on the posteroanterior cephalometric measurements
