3D volume for monitoring the efficacy of methotrexate on placenta accrete: A case report
- Affiliations
-
- 1Department of Obstetrics and Gynecology, The Catholic University of Korea School of Medicine, Seoul, Korea. nigothemo@catholic.ac.kr
- KMID: 2273874
- DOI: http://doi.org/10.5468/kjog.2010.53.5.422
Abstract
- Placenta accreta is a rare condition in which the placenta abnormally attaches to myometrium. It is associated with a high maternal morbidity and mortality rate due to massive hemorrhage, perforation, and infection. It is very rare to have placenta accreta in first trimester. Traditionally, hysterectomy has been the most performed management in abnormal placentation. Because it cannot preserve fertility, the conservative management such as methotrexate usage, and uterine artery embolization are pursued, recently. For monitoring the efficacy of the conservative management, serum human chorionic gonadotrophin (hCG) level has been used, however, low hCG does not always reflect the success of the treatment. 3D-ultrasonography is a new method to pursue the effect of conservative care, by measuring the volume of placenta accreta left in situ. We present a case of a 23-year-old patient with retained placenta accreta following dilatation and curettage, under a successful methotrexate treatment. The effect of methotrexate usage was evaluated by 3D-volume.
Keyword
MeSH Terms
Figure
-

Fig. 1 Initial TVS finding before methotrexate treatment, around 3.4×4.32 cm2 sized mixed echogenic mass with increased blood flow with non-coiling turbulent feature exists in color doppler. The feature differentiates it from uterine arteriovenous malformation. Snowstorm appearance, suggesting cystic space was not noted; therefore gestational trophoblastic disease was ruled out. The mass lesion projects into the myometrial tissue and thinning of the adjacent myometrium is evident, suggesting that it is not just simple remnant placenta.

Fig. 2 2D & 3D TVS finding of remnant placenta after 1st methotrexate injection. The placenta size is 3.38×4.29 cm2 and the volume is 21.597 cm3.
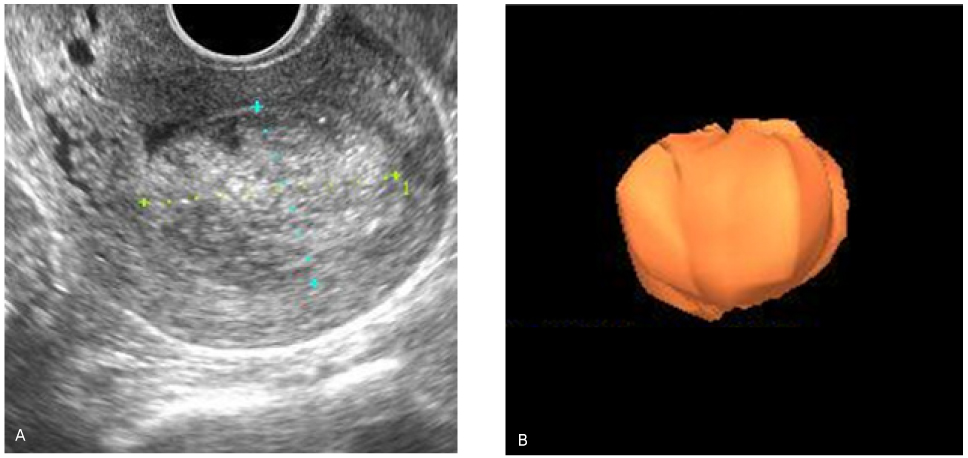
Fig. 3 2D & 3D TVS finding of remnant placenta after 2nd methotrexate injection. The placenta size is 2.8×3.8 cm2 and the volume is 15.849 cm3.
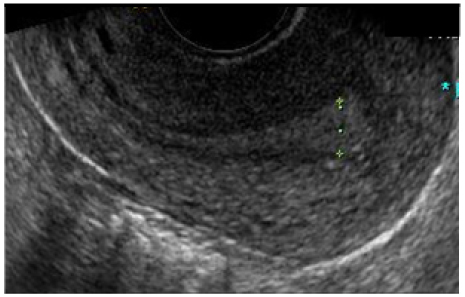
Fig. 4 Follow-up TVS, 2 months after 2 cycles of IM methotrexate and dilatation and curettage. Endometrium thickness is 0.7 cm and no other specific findings are checked.
Reference
-
1. Fox H. Placenta accreta,1945-1969. Obstet Gynecol Surv. 1972. 27:475–490.2. Deka D. First trimester 'retained abortion'-can it be termed 'placenta accreta'? Int J Gynaecol Obstet. 1999. 65:189–190.3. Walter AJ, McCullough AE, Patel MD, Cornella JL. Placenta increta presenting as delayed postabortal hemorrhage. Obstet Gynecol. 1999. 93:846.4. Kayem G, Pannier E, Goffinet F, Grange G, Cabrol D. Fertility after conservative treatment of placenta accreta. Fertil Steril. 2002. 78:637–638.5. Timmermans S, van Hof AC, Duvekot JJ. Conservative management of abnormally invasive placentation. Obstet Gynecol Surv. 2007. 62:529–539.6. Kent A. Management of placenta accreta. Rev Obstet Gynecol. 2009. 2:127–128.7. Cho SH, Bai SW, Kwon JY, Koo JS, Kim SK, Park KH. One case of placenta accreta treated with selective uterine artery embolization followed by methotrexate. Korean J Obstet Gynecol. 2004. 47:795–799.8. ACOG Committee opinion. Number 266, January 2002: placenta accreta. Obstet Gynecol. 2002. 99:169–170.9. Finberg HJ, Williams JW. Placenta accreta: prospective sonographic diagnosis in patients with placenta previa and prior cesarean section. J Ultrasound Med. 1992. 11:333–343.10. Arulkumaran S, Ng CS, Ingemarsson I, Ratnam SS. Medical treatment of placenta accreta with methotrexate. Acta Obstet Gynecol Scand. 1986. 65:285–286.11. Takeda A, Koyama K, Imoto S, Mori M, Nakano T, Nakamura H. Conservative management of placenta increta after first trimester abortion by transcatheter arterial chemoembolization: a case report and review of the literature. Arch Gynecol Obstet. 281:381–386.12. Flam F, Karlstrom PO, Carlsson B, Garoff L. Methotrexate treatment for retained placental tissue. Eur J Obstet Gynecol Reprod Biol. 1999. 83:127–129.13. Lee BK, Kang KH, Rho JH, Oh KY, Yang YS, Hwang IT, et al. A case of placenta accreta successfully treated with methotrexate. Korean J Obstet Gynecol. 2005. 48:446–450.14. Matsumura N, Inoue T, Fukuoka M, Sagawa N, Fujii S. Changes in the serum levels of human chorionic gonadotropin and the pulsatility index of uterine arteries during conservative management of retained adherent placenta. J Obstet Gynaecol Res. 2000. 26:81–87.15. Wehbe SA, Ghulmiyyah LM, Carroll KT, Perloe M, Schwartzberg DG, Sills ES. Correlations from gadopentetate dimeglumine-enhanced magnetic resonance imaging after methotrexate chemotherapy for hemorrhagic placenta increta. Biomagn Res Technol. 2003. 1:3.16. Metzenbauer M, Hafner E, Hoefinger D, Schuchter K, Stangl G, Ogris E, et al. Three-dimensional ultrasound measurement of the placental volume in early pregnancy: method and correlation with biochemical placenta parameters. Placenta. 2001. 22:602–605.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of placenta accreta successfully treated with methotrexate
- A Case of Placenta Increta Successfully Treated with Methotrexate and Misoprostol
- One Case of Placenta Accreta Treated with Selective Uterine Artery Embolization Followed by Methotrexate
- One case of placenta increta successfully treated with methotrexate
- A Case of Placenta Increta in the Uterine Sacculation which was Treated with Conservative Methods
