Preliminary study of Korean orthodontic residents' current concepts and knowledge of cleft lip and palate management
- Affiliations
-
- 1Department of Orthodontics, School of Dentistry, Dental Research Institute, Seoul National University, Seoul, Korea. drwhite@unitel.co.kr
- 2Department of Oral and Maxillofacial Surgery, School of Dentistry, Jeonbuk National University, Jeonju, Korea.
- KMID: 2272258
- DOI: http://doi.org/10.4041/kjod.2012.42.3.100
Abstract
OBJECTIVE
A national survey was conducted to assess orthodontic residents' current concepts and knowledge of cleft lip and palate (CLP) management in Korea.
METHODS
A questionnaire consisting of 7 categories and 36 question items was distributed to 16 senior chief residents of orthodontic department at 11 dental university hospitals and 5 medical university hospitals in Korea. All respondents completed the questionnaires and returned them.
RESULTS
All of the respondents reported that they belonged to an interdisciplinary team. Nineteen percent indicated that they use presurgical infant orthopedic (PSIO) appliances. The percentage of respondents who reported they were 'unsure' about the methods about for cleft repair operation method was relatively high. Eighty-six percent reported that the orthodontic treatment was started at the deciduous or mixed dentition. Various answers were given regarding the amount of maxillary expansion for alveolar bone graft and the estimates of spontaneous or forced eruption of the upper canine. Sixty-seven percent reported use of a rapid maxillary expansion appliance as an anchorage device for maxillary protraction with a facemask. There was consensus among respondents regarding daily wearing time, duration of treatment, and amount of orthopedic force. Various estimates were given for the relapse percentage after maxillary advancement distraction osteogenesis (MADO). Most respondents did not have sufficient experience with MADO.
CONCLUSIONS
These findings suggest that education about the concepts and methods of PSIO and surgical repair, consensus regarding orthodontic management protocols, and additional MADO experience are needed in order to improve the quality of CLP management in Korean orthodontic residents.
MeSH Terms
Figure
-
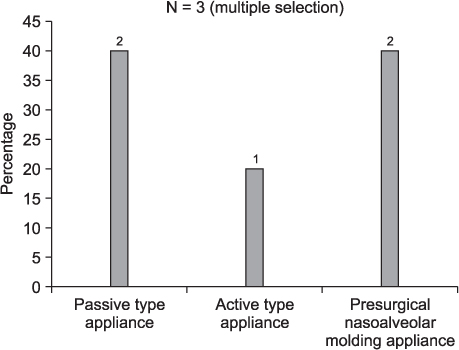
Figure 1 Types of presurgical infant orthopedic appliance.
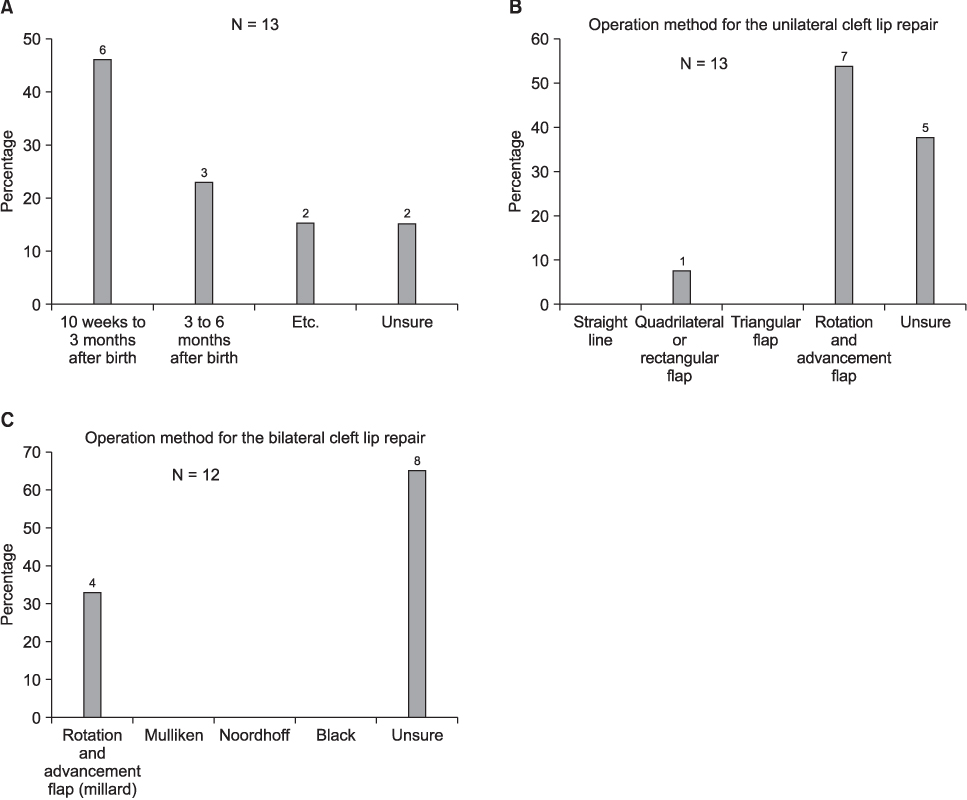
Figure 2 Cleft lip (CL) repair. A, Operation timing; B and C, operation method for unilateral and bilateral CL.

Figure 3 Cleft palate repair. A, Operation timing; B, concept of stage; C, operation method.
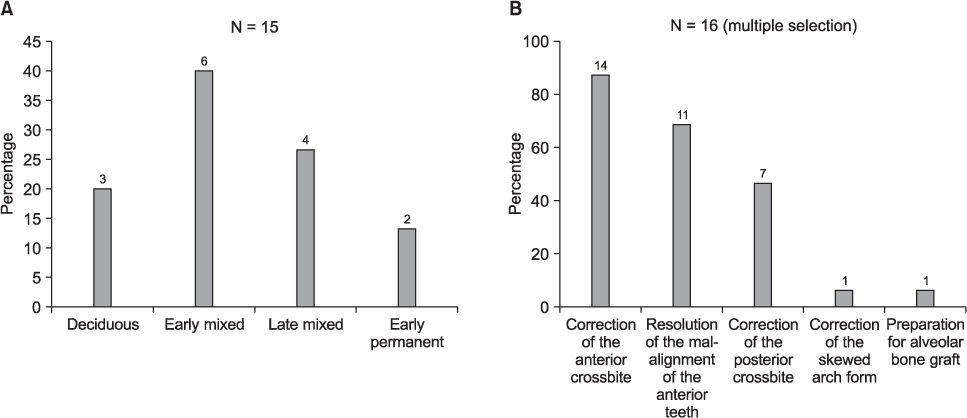
Figure 4 Early orthodontic treatment for cleft patients. A, Timing; B, primary goals.
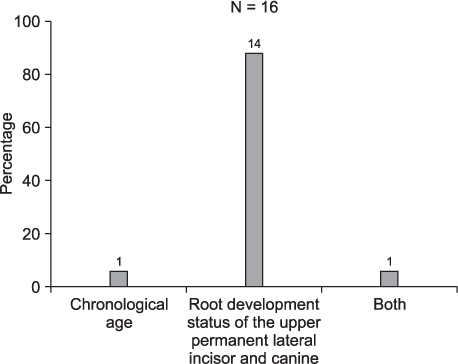
Figure 5 Criteria for the determination of alveolar bone graft timing.
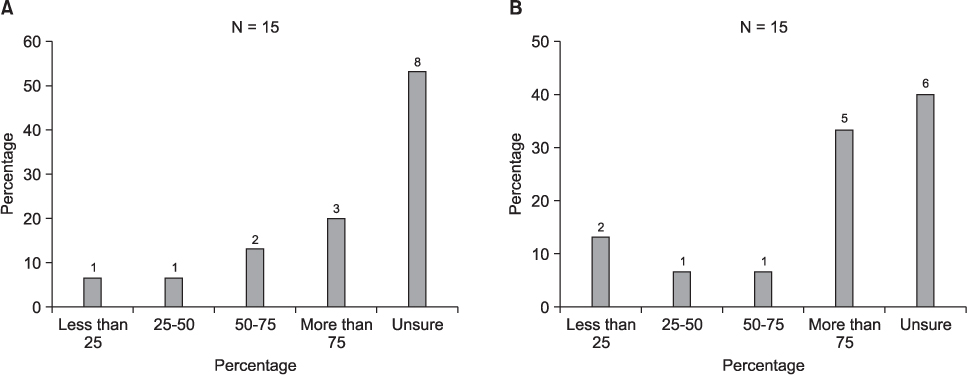
Figure 6 Estimates of the percentage of eruption of the upper permanent canine after alveolar bone grafting. A, Percentage of spontaneous eruption; B, percentage of window opening and forced eruption.
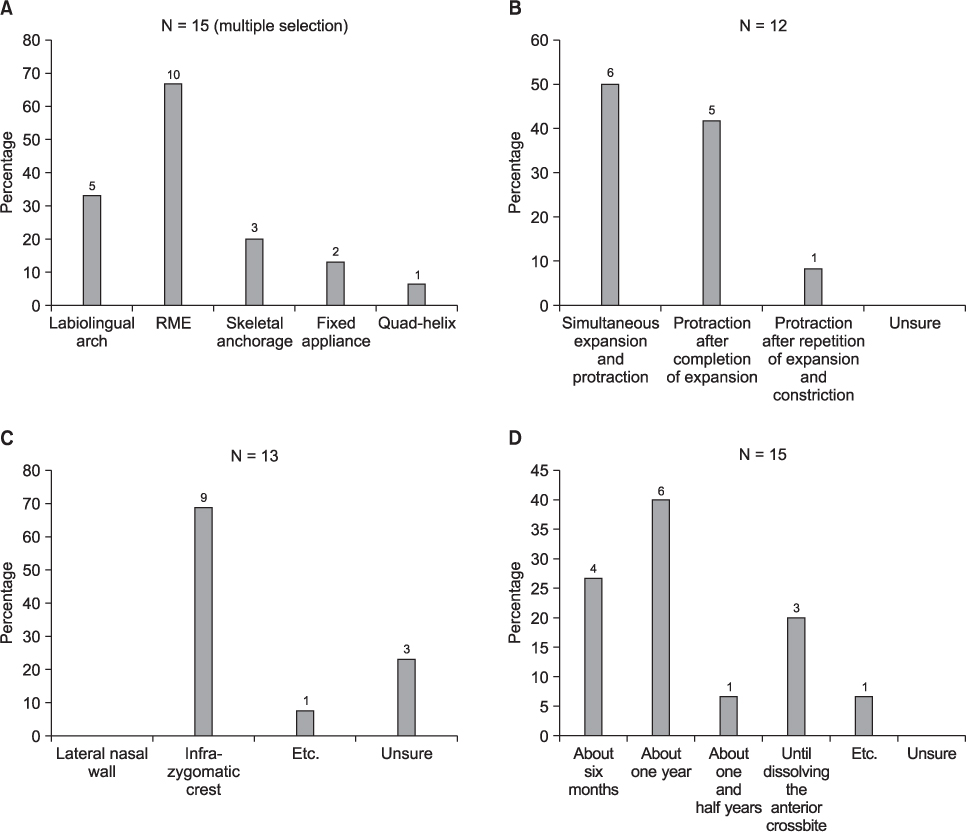
Figure 7 Maxillary protraction with facemask (MP-FM). A, Preferred anchorage device; B, preferred method of the maxillary expansion when using MP-FM with a rapid maxillary expansion appliance; C, preferred site for installation of the skeletal anchorage system; D, average treatment duration. REM, Rapid maxillary expansion.

Figure 8 Surgical correction for cleft patients. A, Timing of maxillary advancement distraction osteogenesis (MADO); B, criteria for differential diagnosis of maxillary advancement with LeFort I osteotomy between conventional orthognathic surgery (COS) and MADO; C, estimates of relapse percentage after COS (gray) and MADO (black); D, estimates of the percentage of cleft patients who require COS and MADO in spite of growth modification.
Reference
-
1. Thornton JB, Nimer S, Howard PS. The incidence, classification, etiology, and embryology of oral clefts. Semin Orthod. 1996. 2:162–168.2. Hongal SG, Ankola A, Nagesh L. Malocclusion and treatment needs of cleft lip and/or palate subjects aged between 12 and 18 years visiting KLE's Hospital, Belgaum, India. Oral Health Prev Dent. 2010. 8:237–242.3. Baek SH, Moon HS, Yang WS. Cleft type and Angle's classification of malocclusion in Korean cleft patients. Eur J Orthod. 2002. 24:647–653.
Article4. Seo YJ, Park JW, Kim YH, Baek SH. Initial growth pattern of children with cleft before alveolar bone graft stage according to cleft type. Angle Orthod. 2011. 81:1103–1110.
Article5. Lewis CW, Ose M, Aspinall C, Omnell ML. Community orthodontists and craniofacial care: results of a Washington state survey. Cleft Palate Craniofac J. 2005. 42:521–525.
Article6. Noble J, Schroth B, Hechter FJ, Huminicki A, Wiltshire WA. Motivations of Orthodontic Residents in Canada and the US to Treat Patients with Craniofacial Anomalies, Cleft Lip/Palate and Special Needs. Cleft Palate Craniofac J. 2011. [Epub ahead of print].7. Osborn JM, Kelleher JC. A survey of cleft lip and palate surgery taught in Plastic Surgery Training Programs. Cleft Palate J. 1983. 20:166–168.8. Brennan PA, Macey-Dare LV, Flood TR, Markus AF, Uppal R. Cleft lip and palate management by U.K. consultant oral and maxillofacial surgeons: a national survey. Cleft Palate Craniofac J. 2001. 38:44–48.
Article9. Weinfeld AB, Hollier LH, Spira M, Stal S. International trends in the treatment of cleft lip and palate. Clin Plast Surg. 2005. 32:19–23.
Article10. Murthy AS, Lehman JA. Evaluation of alveolar bone grafting: a survey of ACPA teams. Cleft Palate Craniofac J. 2005. 42:99–101.
Article11. Eom JS, Lee TJ. Changing trends in cleft lip and palate management taught in training programs in Korea. J Craniofac Surg. 2011. 22:430–433.
Article12. Tang EL, So LL. Prevalence and severity of malocclusion in children with cleft lip and/or palate in Hong Kong. Cleft Palate Craniofac J. 1992. 29:287–291.
Article13. Williams AC, Sandy JR, Shaw WC, Devlin HB. Consultant orthodontic services for cleft patients in England and Wales. Br J Orthod. 1996. 23:165–171.
Article14. Friede H. Maxillary growth controversies after two-stage palatal repair with delayed hard palate closure in unilateral cleft lip and palate patients: perspectives from literature and personal experience. Cleft Palate Craniofac J. 2007. 44:129–136.
Article15. da Silva Filho OG, Teles SG, Ozawa TO, Filho LC. Secondary bone graft and eruption of the permanent canine in patients with alveolar clefts: literature review and case report. Angle Orthod. 2000. 70:174–178.16. Baek SH, Kim KW, Choi JY. New treatment modality for maxillary hypoplasia in cleft patients. Protraction facemask with miniplate anchorage. Angle Orthod. 2010. 80:595–603.17. Saelen R, Tornes K, Halse A. Stability after Le Fort I osteotomy in cleft lip and palate patients. Int J Adult Orthodon Orthognath Surg. 1998. 13:317–323.18. Baek SH, Lee JK, Lee JH, Kim MJ, Kim JR. Comparison of treatment outcome and stability between distraction osteogenesis and LeFort I osteotomy in cleft patients with maxillary hypoplasia. J Craniofac Surg. 2007. 18:1209–1215.
Article19. Posnick JC, Dagys AP. Skeletal stability and relapse patterns after Le Fort I maxillary osteotomy fixed with miniplates: the unilateral cleft lip and palate deformity. Plast Reconstr Surg. 1994. 94:924–932.
Article20. Figueroa AA, Polley JW, Friede H, Ko EW. Long-term skeletal stability after maxillary advancement with distraction osteogenesis using a rigid external distraction device in cleft maxillary deformities. Plast Reconstr Surg. 2004. 114:1382–1392.
Article21. DeLuke DM, Marchand A, Robles EC, Fox P. Facial growth and the need for orthognathic surgery after cleft palate repair: literature review and report of 28 cases. J Oral Maxillofac Surg. 1997. 55:694–697.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Orthodontic consideration of cleft lip and palate (Report 1)
- The prevalence of cleft lip and/or cleft palate in Korean male adult
- Management of Swallowing and Speech Problems in Patients with Cleft Lip and Palate
- The use of classification in primary and secondary cleft lip and nose deformities in medical records
- Cleft Lip and Cleft Palate Patients in Korea
