Ann Surg Treat Res.
2015 Mar;88(3):140-144. 10.4174/astr.2015.88.3.140.
Role of charcoal tattooing in localization of recurred papillary thyroid carcinoma: initial experiences
- Affiliations
-
- 1Department of Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. kyueunlee@snu.ac.kr
- 2Department of Surgery, Ulsan University Hospital, Ulsan University College of Medicine, Ulsan, Korea.
- 3Department of Pathology, Seoul National University Hospital, Seoul National College of Medicine, Seoul, Korea.
- 4Department of Radiology, Seoul National University Hospital, Seoul National College of Medicine, Seoul, Korea.
- 5Department of Surgery, National Medical Center, Seoul, Korea.
- KMID: 2266871
- DOI: http://doi.org/10.4174/astr.2015.88.3.140
Abstract
- PURPOSE
Surgical excision is the definitive treatment for localized recurrence of papillary thyroid carcinoma. Reoperation for recurrence, however, is challenging and associated with increased operative times and complication rates. For safe and effective reoperation, ultrasound-guided charcoal tattooing localization can be used. The aim of this study was to investigate the feasibility and safety of the ultrasound-guided charcoal tattooing localization.
METHODS
Between November 2012 and August 2013, ten patients underwent preoperative charcoal tattooing localization for twelve recurrent lesions. Patient demographics, pathologic features, and operation results were reviewed.
RESULTS
The technical success rate of charcoal tattooing was 100%. Eight patients had one recurrent lesion, and two patients had double lesions. Among these 12 recurrent lesions, three (25%) were found in level II, four (33%) in level IV, four (33%) in level VI, and one (8%) was found in the thyroidectomy bed site. The mean size of lesions was 0.87 +/- 0.35 cm. Of these 10 patients, eight patients underwent selective lymph node dissection, one patient underwent modified radical neck dissection, and one patient underwent recurrent mass excision. Transient hypocalcemia developed in one patient, and no recurrent laryngeal nerve palsy occurred. There were no major complications related to the injection of the charcoal. The mean follow-up period after reoperation was 8.6 +/- 2.7 months; in the follow-up ultrasound, there were no remnant lesions in all patients.
CONCLUSION
Preoperative ultrasound-guided charcoal tattooing localization for recurrent thyroid cancer appears to be a feasible and safe procedure for reoperation. Further evaluation is warranted in larger patients' cohorts.
Keyword
MeSH Terms
Figure
-

Fig. 1 Charcoal injection to localized recurrent lesions under ultrasound guidance. Needle (red arrows) tip was inserted into recurrent lymph node (yellow circle).
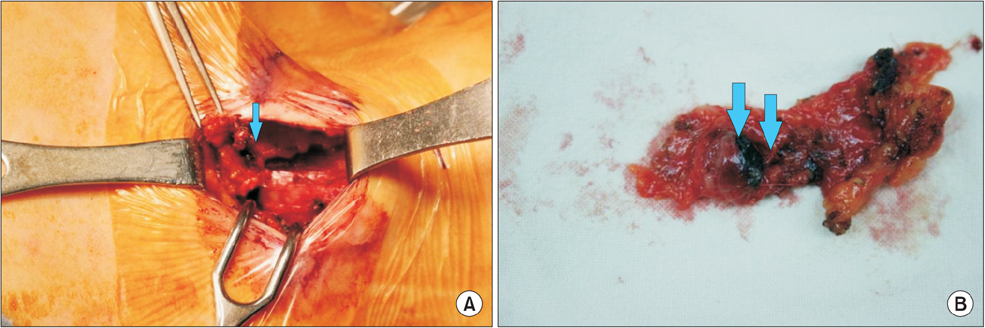
Fig. 2 Charcoal tattooing lesion was easily localized in surgical field and specimen; operation field (A) and resected mass (B). Arrows mark charcoal inside the recurrent lesion.
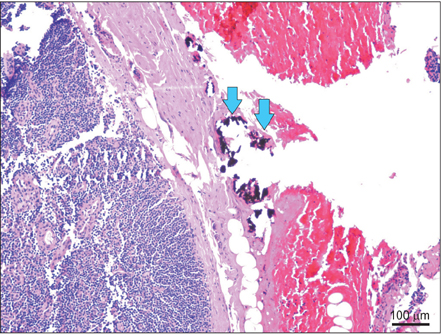
Fig. 3 The charcoal (arrows) was surrounded by collagen fibers; charcoal has no interference with results of pathology (H&E, ×100).
Reference
-
1. Cho BY, Choi HS, Park YJ, Lim JA, Ahn HY, Lee EK, et al. Changes in the clinicopathological characteristics and outcomes of thyroid cancer in Korea over the past four decades. Thyroid. 2013; 23:797–804.2. Jung KW, Park S, Kong HJ, Won YJ, Lee JY, Seo HG, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2009. Cancer Res Treat. 2012; 44:11–24.3. Hartl DM, Chami L, Al Ghuzlan A, Leboulleux S, Baudin E, Schlumberger M, et al. Charcoal suspension tattoo localization for differentiated thyroid cancer recurrence. Ann Surg Oncol. 2009; 16:2602–2608.4. Durante C, Haddy N, Baudin E, Leboulleux S, Hartl D, Travagli JP, et al. Longterm outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy. J Clin Endocrinol Metab. 2006; 91:2892–2899.5. Harari A, Sippel RS, Goldstein R, Aziz S, Shen W, Gosnell J, et al. Successful localization of recurrent thyroid cancer in reoperative neck surgery using ultrasound-guided methylene blue dye injection. J Am Coll Surg. 2012; 215:555–561.6. Lefevre JH, Tresallet C, Leenhardt L, Jublanc C, Chigot JP, Menegaux F. Reoperative surgery for thyroid disease. Langenbecks Arch Surg. 2007; 392:685–691.7. Karwowski JK, Jeffrey RB, McDougall IR, Weigel RJ. Intraoperative ultrasonography improves identification of recurrent thyroid cancer. Surgery. 2002; 132:924–928.8. Duprez R, Lebas P, Marc OS, Mongeois E, Emy P, Michenet P. Preoperative US-guided hook-needle insertion in recurrent lymph nodes of papillary thyroid cancer: a help for the surgeon. Eur J Radiol. 2010; 73:40–42.9. Sippel RS, Elaraj DM, Poder L, Duh QY, Kebebew E, Clark OH. Localization of recurrent thyroid cancer using intraoperative ultrasound-guided dye injection. World J Surg. 2009; 33:434–439.10. Binyousef HM, Alzahrani AS, Al-Sobhi SS, Al SH, Chaudhari MA, Raef HM. Preoperative neck ultrasonographic mapping for persistent/recurrent papillary thyroid cancer. World J Surg. 2004; 28:1110–1114.11. Kim WW, Kim JS, Hur SM, Kim SH, Lee SK, Choi JH, et al. Radioguided surgery using an intraoperative PET probe for tumor localization and verification of complete resection in differentiated thyroid cancer: a pilot study. Surgery. 2011; 149:416–424.12. Kang TW, Shin JH, Han BK, Ko EY, Kang SS, Hahn SY, et al. Preoperative ultrasound-guided tattooing localization of recurrences after thyroidectomy: safety and effectiveness. Ann Surg Oncol. 2009; 16:1655–1659.13. Mathieu MC, Bonhomme-Faivre L, Rouzier R, Seiller M, Barreau-Pouhaer L, Travagli JP. Tattooing breast cancers treated with neoadjuvant chemotherapy. Ann Surg Oncol. 2007; 14:2233–2238.14. Gopalakrishna Iyer N, Shaha AR. Complications of thyroid surgery: prevention and management. Minerva Chir. 2010; 65:71–82.15. Candell L, Campbell MJ, Shen WT, Gosnell JE, Clark OH, Duh QY. Ultrasound-guided methylene blue dye injection for parathyroid localization in the reoperative neck. World J Surg. 2014; 38:88–91.16. Triponez F, Poder L, Zarnegar R, Goldstein R, Roayaie K, Feldstein V, et al. Hook needle-guided excision of recurrent differentiated thyroid cancer in previously operated neck compartments: a safe technique for small, nonpalpable recurrent disease. J Clin Endocrinol Metab. 2006; 91:4943–4947.17. Rubello D, Salvatori M, Casara D, Piotto A, Toniato A, Gross MD, et al. 99mTcsestamibi radio-guided surgery of locoregional 131Iodine-negative recurrent thyroid cancer. Eur J Surg Oncol. 2007; 33:902–906.18. Rubello D, Salvatori M, Ardito G, Mariani G, Al-Nahhas A, Gross MD, et al. Iodine-131 radio-guided surgery in differentiated thyroid cancer: outcome on 31 patients and review of the literature. Biomed Pharmacother. 2007; 61:477–481.19. Travagli JP, Cailleux AF, Ricard M, Baudin E, Caillou B, Parmentier C, et al. Combination of radioiodine (131I) and probeguided surgery for persistent or recurrent thyroid carcinoma. J Clin Endocrinol Metab. 1998; 83:2675–2680.20. Naveau S, Bonhomme L, Preaux N, Chaput JC. A pure charcoal suspension for colonoscopic tattoo. Gastrointest Endosc. 1991; 37:624–625.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Concurrent Medullay and Papillary Carcinoma of the Thyroid
- A Case of Concurrent Papillary and Medullary Thyroid Carcinomas Detected as Recurrent Medullary Carcinoma after Initial Surgery for Papillary Carcinoma
- Effectiveness of preoperative ultrasound-guided charcoal tattooing for localization of metastatic melanoma
- A Case of Ectopic Thyroid Papillary Carcinoma with Incidental Papillary Thyroid Microcarcinoma
- Preoperative Colonoscopic Tattooing with Autologous Blood in Laparoscopic Colorectal Cancer Surgery: Red-Flagging for an Invisible Enemy
