Ann Rehabil Med.
2013 Aug;37(4):563-566. 10.5535/arm.2013.37.4.563.
Adrenomyeloneuropathy Presenting With Adrenal Insufficiency
- Affiliations
-
- 1Department of Rehabilitation Medicine, Seoul Medical Center, Seoul, Korea. wisdom1409@hanmail.net
- KMID: 2266613
- DOI: http://doi.org/10.5535/arm.2013.37.4.563
Abstract
- Adrenomyeloneuropathy (AMN), one of the variants of X-linked adrenoleukodystrophy (ALD), is inherited peroxisomal disorder associated with the accumulation of very long chain fatty acids (VLCFA). AMN is characterized primarily by involvements of long ascending and descending tracts of the spinal cord and peripheral neuropathy, which leads to spastic paraparesis and urinary and erectile dysfunction. We experienced the AMN case of a 33-year-old man presenting bilateral progressive spastic paraparesis, impotence and urge incontinence with primary adrenal failures, as confirmed by increased serum of VLCFA concentrations. Considering that somatosensory evoked potentials in posterior tibial nerve was the only abnormal finding in electrophysiologic findings when compared with the severe spastic gait pattern shown, it is necessary to follow up with electrophysiologic studies.
MeSH Terms
Figure
-
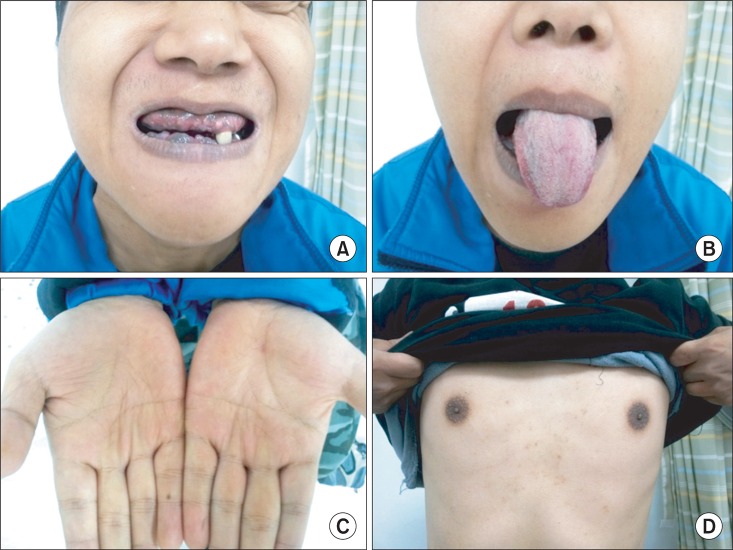
Fig. 1 The patient shows hyperpigmentation in gingiva (A), tongue (B), creases of hand (C), and areolae (D).
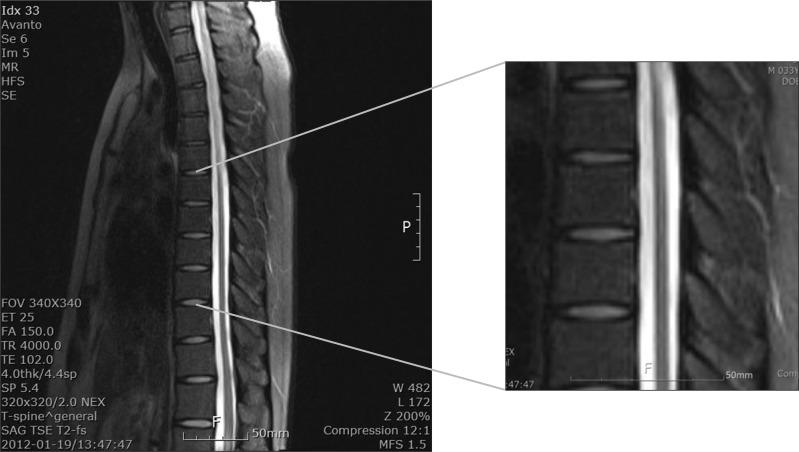
Fig. 2 T-spine magnetic resonance imaging shows a T2-weighted sagittal image of intramedullary signal changes along entire thoracic cord, which are suggestive of myelopathy.
Reference
-
1. Spurek M, Taylor-Gjevre R, Van Uum S, Khandwala HM. Adrenomyeloneuropathy as a cause of primary adrenal insufficiency and spastic paraparesis. CMAJ. 2004; 171:1073–1077. PMID: 15505272.
Article2. Moser HW, Raymond GV, Dubey P. Adrenoleukodystrophy: new approaches to a neurodegenerative disease. JAMA. 2005; 294:3131–3134. PMID: 16380594.3. Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J. Harrison's principles of internal medicine. 18th ed. New York: McGraw-Hill;2011.4. Zelissen PM, Bast EJ, Croughs RJ. Associated autoimmunity in Addison's disease. J Autoimmun. 1995; 8:121–130. PMID: 7734032.
Article5. Sung SK, Kwon YJ, Lee BW, Kim DM, Yoo HJ. Clinical review of Addison's disease in Korea previously reported 14 cases in Korea and 6 new cases at National Medical Center. J Korean Soc Endocrinol. 1987; 2:189–193.6. Powers JM, Schaumburg HH. The testis in adreno-leukodystrophy. Am J Pathol. 1981; 102:90–98. PMID: 7468762.7. Sadeghi-Nejad A, Senior B. Adrenomyeloneuropathy presenting as Addison's disease in childhood. N Engl J Med. 1990; 322:13–16. PMID: 2294415.
Article8. Dumitru D, Amato AA, Zwarts MJ. Electrodiagnostic medicine. 2nd ed. Philadelphia: Hanley & Belfus;2002.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Adrenomyeloneuropathy
- A Case of Primary Adrenal Insufficiency Presenting as the Initial Clinical Manifestation of Primary Antiphospholipid Antibody Syndrome
- Novel ABCD1 Gene Mutation in a Korean Patient with X-Linked Adrenoleukodystrophy Presenting with Addison's Disease
- Adrenal Tuberculosis Mimicking a Malignant Tumor with Primary Adrenal Insufficiency
- A Case of Adrenal Aplasia
