Ann Rehabil Med.
2013 Oct;37(5):735-739. 10.5535/arm.2013.37.5.735.
Supplementary Motor Area Syndrome and Flexor Synergy of the Lower Extremities
- Affiliations
-
- 1Department of Rehabilitation Medicine, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- 2Department of Rehabilitation Medicine, Asan Medical Center, University of Ulsan Collage of Medicine, Seoul, Korea. mhchun@amc.seoul.kr
- KMID: 2266595
- DOI: http://doi.org/10.5535/arm.2013.37.5.735
Abstract
- Clinical presentation of supplementary motor area (SMA) syndrome includes complete akinesia of the contralateral side of the body and mutism, with secondary recovery of neurologic deficit. Multi-joint coordination is frequently impaired following the development of a brain lesion and is generally restricted by abnormal patterns of muscle activation within the hemiparetic limb, clinically termed muscle synergies. However, no work to date has confirmed this observation with the aid of objective methods, such as gait analysis, and the development of reflex pattern has not been suggested as a possible cause. We describe two unusual cases of flexor synergy after tumor resection of SMA lesions.
Keyword
MeSH Terms
Figure
-
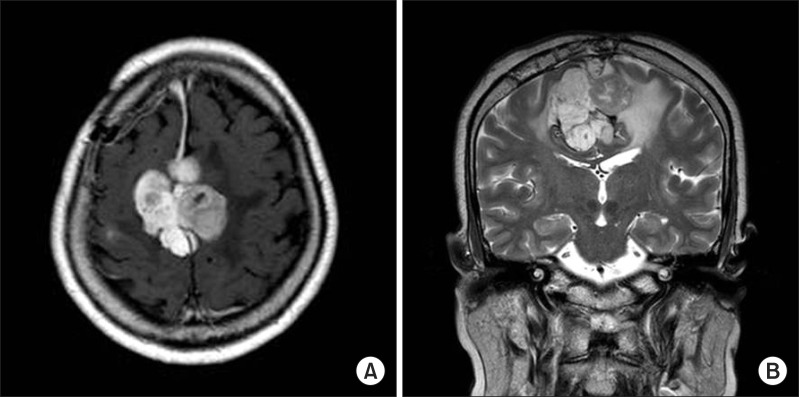
Fig. 1 Enhanced brain magnetic resonance imaging of patient (case 1): (A) coronal view and (B) sagittal view.

Fig. 2 Gait analysis of patient 1 (a solid line, right side; a dotted line, left side). Pos, posterior; Ant, anterior; Ext, extention; Flx, flexion; Pla, planta flexion; Dor, dorsiflexion.

Fig. 3 T2-weighted brain magnetic resonance imaging of patient 2: (A) coronal view and (B) sagittal view.

Fig. 4 Gait analysis of patient 2 (a solid line, right side; a dotted line, left side). Pos, posterior; Ant, anterior; Ext, extention; Flx, flexion; Pla, planta flexion; Dor, dorsiflexion.
Reference
-
1. Penfield W, Welch K. The supplementary motor area of the cerebral cortex; a clinical and experimental study. AMA Arch Neurol Psychiatry. 1951; 66:289–317.2. Dewald JP, Beer RF. Abnormal joint torque patterns in the paretic upper limb of subjects with hemiparesis. Muscle Nerve. 2001; 24:273–283. PMID: 11180211.
Article3. Trumbower RD, Ravichandran VJ, Krutky MA, Perreault EJ. Altered multijoint reflex coordination is indicative of motor impairment level following stroke. Conf Proc IEEE Eng Med Biol Soc. 2008; 2008:3558–3561. PMID: 19163477.
Article4. Aruin AS. Simple lower extremity two-joint synergy. Percept Mot Skills. 2001; 92:563–568. PMID: 11361322.
Article5. Russell SM, Kelly PJ. Incidence and clinical evolution of postoperative deficits after volumetric stereotactic resection of glial neoplasms involving the supplementary motor area. Neurosurgery. 2007; 61(1 Suppl):358–367. PMID: 18813154.
Article6. Fontaine D, Capelle L, Duffau H. Somatotopy of the supplementary motor area: evidence from correlation of the extent of surgical resection with the clinical patterns of deficit. Neurosurgery. 2002; 50:297–303. PMID: 11844264.
Article7. Bannur U, Rajshekhar V. Postoperative supplementary motor area syndrome: clinical features and outcome. Br J Neurosurg. 2000; 14:204–210. PMID: 10912196.8. Duffau H, Lopes M, Denvil D, Capelle L. Delayed onset of the supplementary motor area syndrome after surgical resection of the mesial frontal lobe: a time course study using intraoperative mapping in an awake patient. Stereotact Funct Neurosurg. 2001; 76:74–82. PMID: 12007269.
Article9. Nudo RJ, Plautz EJ, Frost SB. Role of adaptive plasticity in recovery of function after damage to motor cortex. Muscle Nerve. 2001; 24:1000–1019. PMID: 11439375.
Article10. Thilmann AF, Fellows SJ, Garms E. The mechanism of spastic muscle hypertonus: variation in reflex gain over the time course of spasticity. Brain. 1991; 114:233–244. PMID: 1998884.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Periodic Limb Movement and Restless legs Syndrome in Neurological Disorders
- Functional MRI of The Supplementary Motor Area in Hand Motor Task: Comparison Study with The Primary Motor Area
- The Anterior Interosseous Nerve Syndrome
- Cortical Activation Related to Motor and Sensory Tasks in Congenital Mirror Movement using Functional MRI
- Mirror-writing after Corpus Callosum Lesion Induced by Both Posterior Cerebral Artery Infarction: A case report
