Ann Rehabil Med.
2014 Feb;38(1):127-131. 10.5535/arm.2014.38.1.127.
Effects of Botulinum Toxin on Reducing the Co-contraction of Antagonists in Birth Brachial Plexus Palsy
- Affiliations
-
- 1Department of Rehabilitation Medicine, Pusan National University School of Medicine, Busan, Korea. drshinmj@gmail.com
- 2Biomedical Research Institute, Pusan National University Hospital, Busan, Korea.
- 3Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea.
- KMID: 2266551
- DOI: http://doi.org/10.5535/arm.2014.38.1.127
Abstract
- Birth brachial plexus palsy (BBPP) is usually caused by plexus traction during difficult delivery. Although the possibility of complete recovery is relatively high, 5% to 25% of BBPP cases result in prolonged and persistent disability. In particular, muscle imbalance and co-contraction around the shoulder and elbow cause abnormal motor performance, osseous deformities, and joint contracture. Physical and occupational therapies have most commonly been used, but these conventional therapeutic strategies have often been inadequate, in managing the residual muscle imbalance and muscle co-contraction. Therefore, we attempted to improve the functional movements, by using botulinum toxin type A, to reduce the abnormal co-contraction of the antagonist muscles.
Keyword
MeSH Terms
Figure
-

Fig. 1 Participant flow chart. BTX, botulinum toxin type A.
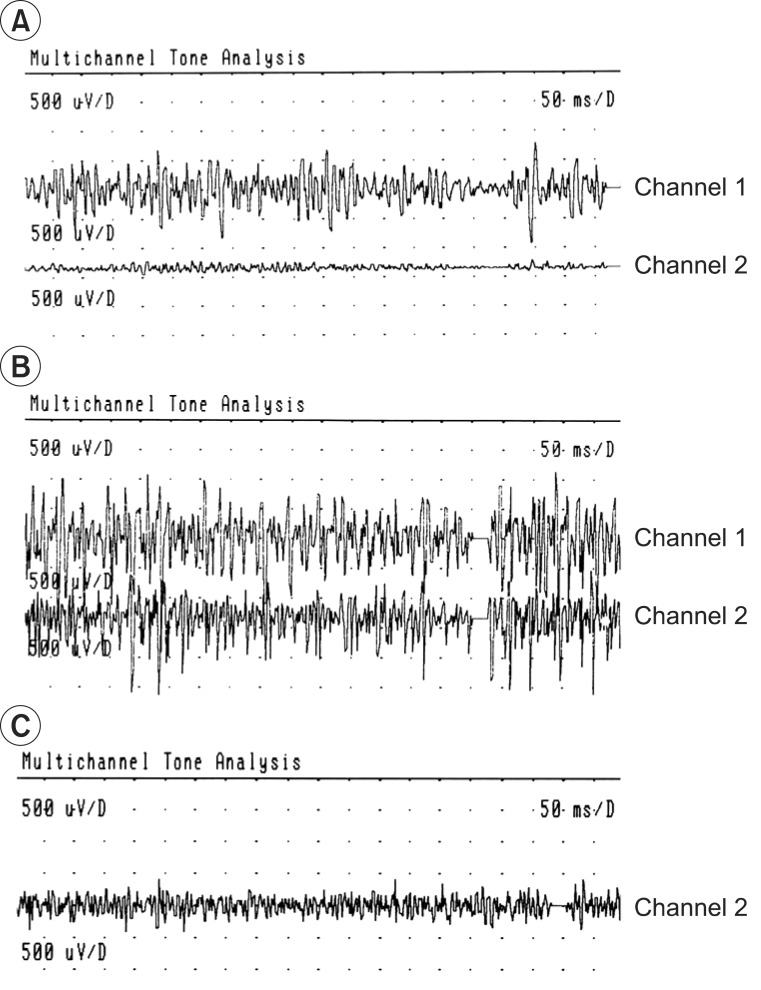
Fig. 2 Two channels surface electromyography of biceps (channel 1) and triceps (channel 2) muscles. (A) Normal contraction pattern of the biceps and triceps muscles during elbow flexion on sound side, before the use of botulinum toxin type A (BTA). (B) The biceps-triceps co-contraction and the pronounced triceps activation during elbow flexion on involved side, before the use of BTA. (C) Reduced triceps co-contraction, 3 weeks after the injection of the BTA in the triceps muscle (only channel 2 visible).
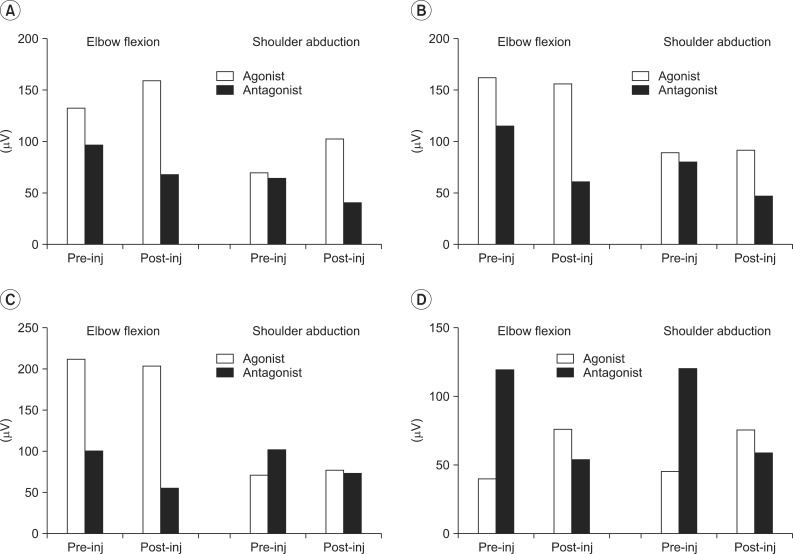
Fig. 3 Root mean square changes after botulinum toxin type A injection. (A) Case 1, (B) case 2, (C) case 3, and (D) case 4.
Reference
-
1. van Dijk JG, Pondaag W, Malessy MJ. Obstetric lesions of the brachial plexus. Muscle Nerve. 2001; 24:1451–1461. PMID: 11745946.
Article2. Brown T, Cupido C, Scarfone H, Pape K, Galea V, McComas A. Developmental apraxia arising from neonatal brachial plexus palsy. Neurology. 2000; 55:24–30. PMID: 10891898.
Article3. Vekris MD, Lykissas MG, Beris AE, Manoudis G, Vekris AD, Soucacos PN. Management of obstetrical brachial plexus palsy with early plexus microreconstruction and late muscle transfers. Microsurgery. 2008; 28:252–261. PMID: 18381657.
Article4. DeMatteo C, Bain JR, Galea V, Gjertsen D. Botulinum toxin as an adjunct to motor learning therapy and surgery for obstetrical brachial plexus injury. Dev Med Child Neurol. 2006; 48:245–252. PMID: 16542510.
Article5. Pearl ML. Shoulder problems in children with brachial plexus birth palsy: evaluation and management. J Am Acad Orthop Surg. 2009; 17:242–254. PMID: 19307673.
Article6. Strömbeck C, Krumlinde-Sundholm L, Forssberg H. Functional outcome at 5 years in children with obstetrical brachial plexus palsy with and without microsurgical reconstruction. Dev Med Child Neurol. 2000; 42:148–157. PMID: 10755453.
Article7. van Dijk JG, Pondaag W, Malessy MJ. Botulinum toxin and the pathophysiology of obstetric brachial plexus lesions. Dev Med Child Neurol. 2007; 49:318. PMID: 17376145.8. Intiso D, Basciani M. Botulinum toxin use in neuro-rehabilitation to treat obstetrical plexus palsy and sialorrhea following neurological diseases: a review. NeuroRehabilitation. 2012; 31:117–129. PMID: 22951705.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Phrenic nerve palsy following coracoid infraclavicular brachial plexus block
- Effects of Botulinum Toxin A Treatment in Cerebral Palsy
- Delayed Brachial Plexus Palsy due to Clavicular Fracture: A Case Report
- Pyogenic Arthritis of the Shoulder Associated with Brachial Plexus Palsy: A Case Report
- Progressive Brachial Plexus Palsy after Fixation of Clavicle Shaft Nonunion: A Case Report
