Occipital Condyle Fracture With Isolated Unilateral Hypoglossal Nerve Palsy
- Affiliations
-
- 1Department of Physical & Rehabilitation Medicine, Gachon University School of Medicine, Incheon, Korea. pmrdoc@gilhospital.com
- KMID: 2266504
- DOI: http://doi.org/10.5535/arm.2014.38.5.689
Abstract
- Occipital condyle fractures (OCFs) with selective involvement of the hypoglossal canal are rare. OCFs usually occur after major trauma and combine multiple fractures. We describe a 38-year-old man who presented with neck pain and a tongue deviation to the right side after a traffic accident. Severe limitations were detected during active and passive range of neck motion in all directions. A physical examination revealed a normal gag reflex and normal mobility of the palate, larynx, and shoulder girdle. He had normal taste and general sensation in his tongue. However, he presented with a tongue deviation to the right side on protrusion. A videofluoroscopic swallowing study revealed piecemeal deglutition due to decreased tongue mobility but no aspiration of food. Plain X-ray film findings were negative, but a computed tomography study with coronal reconstruction demonstrated a right OCF involving the hypoglossal canal. An electrodiagnostic study revealed evidence of right hypoglossal nerve palsy. We report a rare case of isolated hypoglossal nerve palsy caused by an OCF.
Keyword
MeSH Terms
Figure
-
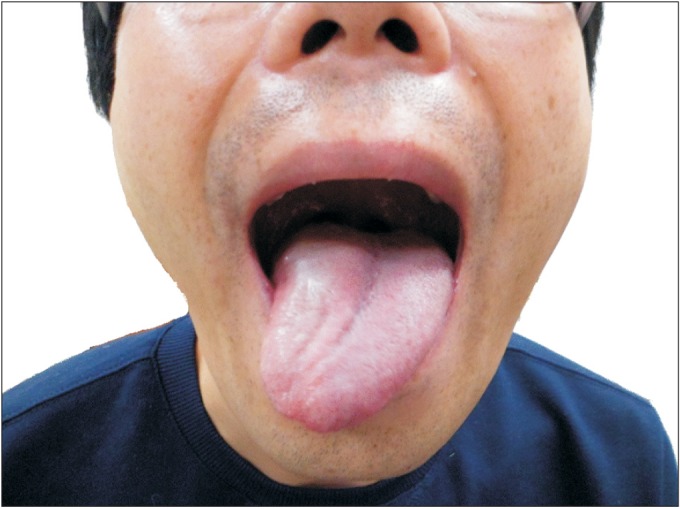
Fig. 1 Tongue deviates to the right side on protrusion, and it is atrophied on the right side.
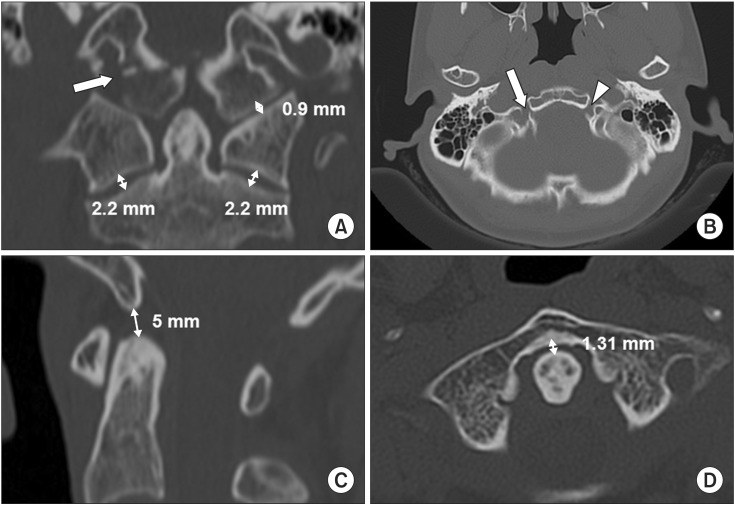
Fig. 2 (A) Computed tomography scan reveals an Anderson and Montesano type III occipital condyle fracture (arrow) and no widening of the occipitoatlantal or atlantoaxial joints. (B) The occipital condyle fracture involves the right hypoglossal canal (arrow) but the left hypoglossal canal is intact (arrowhead). Structural stability of the craniocervical joints is maintained with (C) a basiondens interval of 5 mm and (D) an anterior atlanto-dens interval of 1.31 mm.
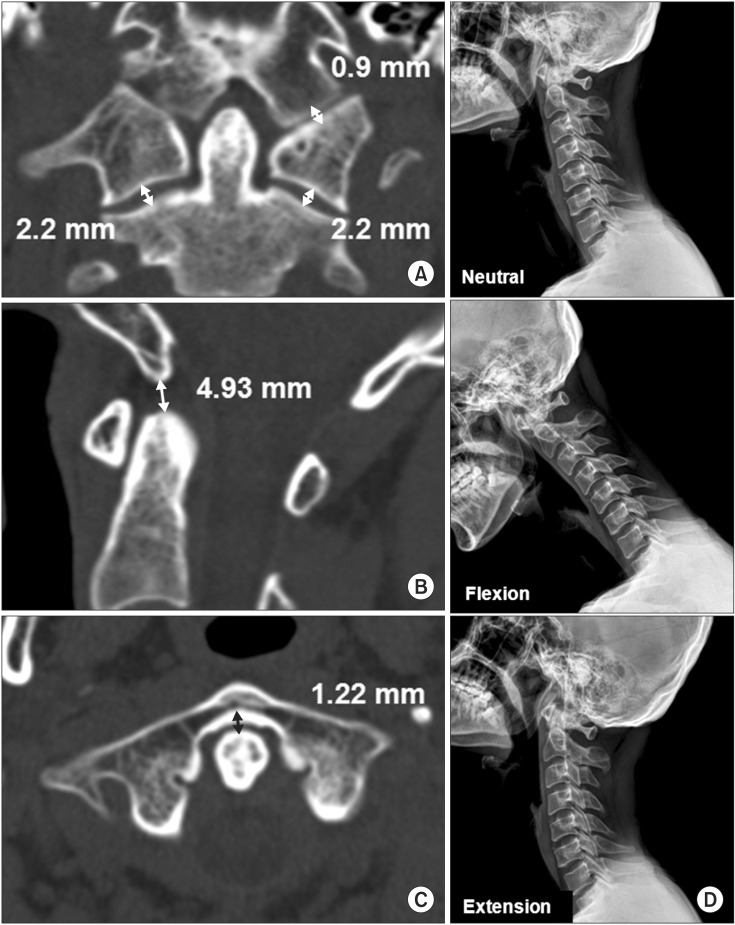
Fig. 3 Follow-up computed tomography (CT) scan and plain X-ray performed 16 weeks after the motor vehicle crash. (A) The CT scan reveals structural stability of craniocervical joints with no widening of the occipitoatlantal or atlantoaxial joints. (B) Basiondens interval of 4.93 mm and (C) anterior atlanto-dens interval of 1.22 mm. (D) Lateral view cervical radiograph shows structural stability of the craniocervical joints.
Reference
-
1. Anderson PA, Montesano PX. Morphology and treatment of occipital condyle fractures. Spine (Phila Pa 1976). 1988; 13:731–736. PMID: 3194779.
Article2. Tuli S, Tator CH, Fehlings MG, Mackay M. Occipital condyle fractures. Neurosurgery. 1997; 41:368–377. PMID: 9257304.
Article3. Kaushik V, Kelly G, Richards SD, Saeed SR. Isolated unilateral hypoglossal nerve palsy after minor head trauma. Clin Neurol Neurosurg. 2002; 105:42–47. PMID: 12445924.
Article4. Choi HK, Chung BS, Shin MS. Delayed hypoglossal nerve palsy following fracture of the occipital condyle. J Korean Neurosurg Soc. 1998; 27:403–406.5. Hanson JA, Deliganis AV, Baxter AB, Cohen WA, Linnau KF, Wilson AJ, et al. Radiologic and clinical spectrum of occipital condyle fractures: retrospective review of 107 consecutive fractures in 95 patients. AJR Am J Roentgenol. 2002; 178:1261–1268. PMID: 11959743.6. Song KJ, Choi BW, Kim SJ, Yoon SJ. Cross-cultural adaptation and validation of the Korean version of the Neck Disability Index. J Korean Orthop Assoc. 2009; 44:350–359.
Article7. Maddox JJ, Rodriguez-Feo JA 3rd, Maddox GE, Gullung G, McGwin G, Theiss SM. Nonoperative treatment of occipital condyle fractures: an outcomes review of 32 fractures. Spine (Phila Pa 1976). 2012; 37:E964–E968. PMID: 22414996.8. Caroli E, Rocchi G, Orlando ER, Delfini R. Occipital condyle fractures: report of five cases and literature review. Eur Spine J. 2005; 14:487–492. PMID: 15754215.
Article9. Maserati MB, Stephens B, Zohny Z, Lee JY, Kanter AS, Spiro RM, et al. Occipital condyle fractures: clinical decision rule and surgical management. J Neurosurg Spine. 2009; 11:388–395. PMID: 19929333.
Article10. Mueller FJ, Fuechtmeier B, Kinner B, Rosskopf M, Neumann C, Nerlich M, et al. Occipital condyle fractures: prospective follow-up of 31 cases within 5 years at a level 1 trauma centre. Eur Spine J. 2012; 21:289–294. PMID: 21833573.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Delayed Hypoglossal Nerve Palsy Following Fracture of the Occipital Condyle: Case Report
- Idiopathic Isolated Hypoglossal Nerve Palsy After Upper Respiratory Infection
- A Case of Occipital Condyle Syndrome Associated with Hepatocellular Carcinoma
- A Case of Improved Idiopathic Isolated Hypoglossal Nerve Palsy without Use of Steroid
- Delayed Isolated Hypoglossal Nerve Palsy after Submandibular Gland Surgery
