Novel Photopneumatic Therapy for the Treatment of Rosacea
- Affiliations
-
- 1Department of Dermatology, Seoul National University College of Medicine, Seoul, Korea.
- 2S&U Clinic, Seoul, Korea. dermkbs@netsgo.com
- KMID: 2266288
- DOI: http://doi.org/10.5021/ad.2009.21.3.268
Abstract
-
BACKGROUND: Rosacea is a common skin condition, but the currently available treatments are not satisfactory.
OBJECTIVE
We wanted to assess the efficacy and safety of photopneumatic therapy (PPx), which delivers pneumatic energy and broadband light (400~1,200 nm), for the treatment of erythematotelangiectatic rosacea.
METHODS
Twenty two patients with erythematotelangiectatic rosacea were treated 3~5 times with PPx. Three independent dermatologists evaluated the efficacy of PPx by comparing the photographs taken before and after treatment. Patient self-assessment was also done by interviews.
RESULTS
The photographic assessment by the dermatologists of the improvement showed that >50% improvement occurred in 64% (14/22) of the patients. The specific categories of improvement were as follows: poor (<25% improvement), 1 patient; fair (25~50% improvement), 7 patients; good (50~75% improvement), 11 patients; and excellent (>75% improvement), 3 patients. Based on the patients' self-assessment, 20 patients (91%) acknowledged an improvement.
CONCLUSION
PPx is an effective and safe treatment option for erythematotelangiectatic rosacea.
Keyword
MeSH Terms
Figure
-
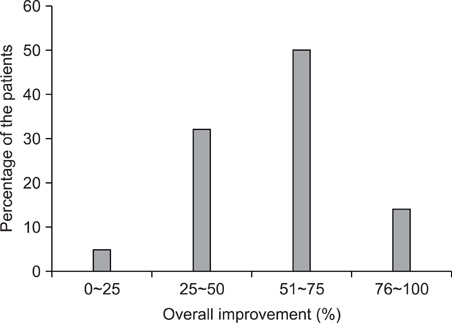
Fig. 1 Percentage of the patients showing different degrees of improvement based on independent photographic evaluation.
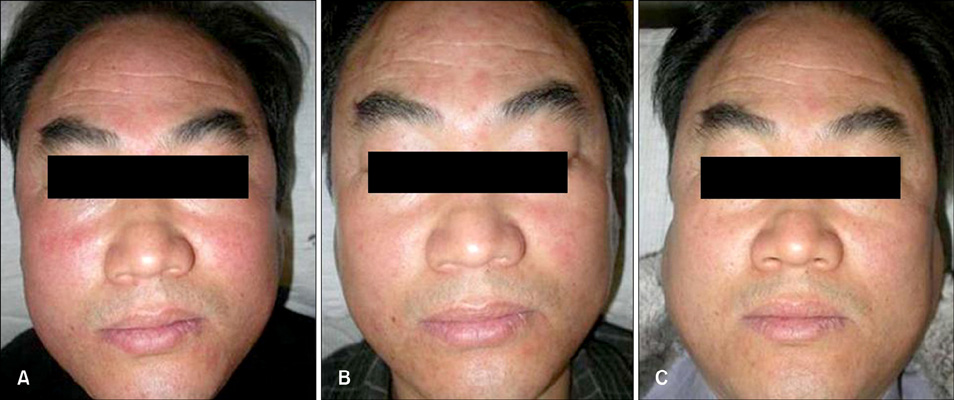
Fig. 2 The clinical pictures of patient 2. (A) Before treatment, (B) 3 weeks after 2 sessions of treatment (right side only [the face was divided into 2 areas]) and (C) 3 months after 5 sessions of treatment to the entire face.

Fig. 3 The clinical pictures of patient 9. (A) Before treatment, (B) 3 weeks after 2 sessions of treatment (right side only [the face was divided into 2 areas]) and (C) 4 months after 5 sessions of treatment to the entire face.

Fig. 4 The clinical pictures of patient 15. (A) Before treatment, (B) 1 month after 1 session of treatment and (C) 1 month after 2 sessions of treatment to the perinasal area.

Fig. 5 Purpura developed on the forehead and the periocular area, and this resolved within 1 week.
Reference
-
1. Plewig G, Jansen T. Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, editors. Rosacea. Fitzpatrick's dermatology in general medicine. 2003. 6th ed. New York: McGraw-Hill;688–696.2. Wilkin J, Dahl M, Detmar M, Drake L, Feinstein A, Odom R, et al. Standard classification of rosacea: report of the National Rosacea Society Expert Committee on the classification and staging of rosacea. J Am Acad Dermatol. 2002. 46:584–587.
Article3. Wilkin J, Dahl M, Detmar M, Drake L, Liang MH, Odom R, et al. Standard grading system for rosacea: report of the National Rosacea Society Expert Committee on the classification and staging of rosacea. J Am Acad Dermatol. 2004. 50:907–912.
Article4. Wilkin JK. Rosacea. Pathophysiology and treatment. Arch Dermatol. 1994. 130:359–362.
Article5. Pelle MT, Crawford GH, James WD. Rosacea: II. Therapy. J Am Acad Dermatol. 2004. 51:499–512.
Article6. Papageorgiou P, Clayton W, Norwood S, Chopra S, Rustin M. Treatment of rosacea with intense pulsed light: significant improvement and long-lasting results. Br J Dermatol. 2008. 159:628–632.
Article7. Lowe NJ, Behr KL, Fitzpatrick R, Goldman M, Ruiz-Esparza J. Flash lamp pumped dye laser for rosacea-associated telangiectasia and erythema. J Dermatol Surg Oncol. 1991. 17:522–525.8. Narurkar VA. Noble photopneumatic therapy delivers high-efficiency photons to dermal targets. Cosmet Dermatol. 2005. 18:115–120.9. West TB, Alster TS. Comparison of the long-pulse dye (590-595 nm) and KTP (532 nm) lasers in the treatment of facial and leg telangiectasias. Dermatol Surg. 1998. 24:221–226.
Article10. Schroeter CA, Haaf-von Below S, Neumann HA. Effective treatment of rosacea using intense pulsed light systems. Dermatol Surg. 2005. 31:1285–1289.
Article11. Mark KA, Sparacio RM, Voigt A, Marenus K, Sarnoff DS. Objective and quantitative improvement of rosacea-associated erythema after intense pulsed light treatment. Dermatol Surg. 2003. 29:600–604.
Article12. Taub AF. Treatment of rosacea with intense pulsed light. J Drugs Dermatol. 2003. 2:254–259.13. Omi T, Munavalli GS, Kawana S, Sato S. Ultrastructural evidence for thermal injury to pilosebaceous units during the treatment of acne using photopneumatic (PPX) therapy. J Cosmet Laser Ther. 2008. 10:7–11.
Article14. Gold MH, Biron J. Efficacy of a novel combination of pneumatic energy and broadband light for the treatment of acne. J Drugs Dermatol. 2008. 7:639–642.15. Shamban AT, Enokibori M, Narurkar V, Wilson D. Photopneumatic technology for the treatment of acne vulgaris. J Drugs Dermatol. 2008. 7:139–145.16. Zelickson B, Kist D. Effect of pulsed dye laser and intense pulsed light source on the dermal extracellular matrix remodeling. Lasers Surg Med. 2000. 12:17.17. Neumann E, Frithz A. Capillaropathy and capillaroneogenesis in the pathogenesis of rosacea. Int J Dermatol. 1998. 37:263–266.
Article18. Gupta AK, Chaudhry MM. Rosacea and its management: an overview. J Eur Acad Dermatol Venereol. 2005. 19:273–285.
Article19. Shin JB, Kim IH. A clinical study of 90 patients with rosacea. Korean J Dermatol. 2007. 45:1161–1169.20. Lee SY, Choi JH, Sung KJ, Moon KC, Koh JK. A clinical study of 112 patients with rosacea. Korean J Dermatol. 2001. 39:636–642.21. Kim TH, Hwang SM, Lee WS, Ahn SK, Choi EH. A clinical study of rosacea. Korean J Dermatol. 2000. 38:583–588.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Ocular Rosacea
- A Comparative Study of Metronidazole Versus Tetracycline Therapy for Rosacea with Demodex folliculorum
- A Rosacea Case Involving One Side of the Face Accompanied by Demodex Infestation: Unilateral Rosacea Fulminans
- An Open-Label, Split-Face Trial Evaluating Efficacy and Safty of Photopneumatic Therapy for the Treatment of Acne
- Rosacea: Clinical Study of 67 Cases
