Role of CD4(+)CD25(high+)FOXP3(+) Regulatory T Cells in Psoriasis
- Affiliations
-
- 1Cleanup Dermatology Clinic, Seoul, Korea.
- 2Department of Dermatology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jhchoy@amc.seoul.kr
- 3Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 4Department of Pathology, Kyungpook National University School of Medicine, Daegu, Korea.
- 5Department of Emergency Medicine, Chung-Ang University College of Medicine, Seoul, Korea.
- 6Department of Dermatology, Chung-Ang University College of Medicine, Seoul, Korea.
- KMID: 2266175
- DOI: http://doi.org/10.5021/ad.2010.22.4.397
Abstract
- BACKGROUND
CD4(+)CD25(high+)regulatory T cells (Tregs) are considered to be of vital importance for maintaining immunologic self-tolerance and preventing autoimmune diseases. These cells have been found to be deficient in skin lesions and in the peripheral blood of patients with psoriasis.
OBJECTIVE
To investigate the role of Tregs in the pathogenesis of psoriasis and to evaluate the changes in Tregs in relation to the severity and the clinical course of psoriasis.
METHODS
Immunohistochemistry (CD3, 4, 8, 79 and FOXP3) was performed in 22 psoriatic patients compared to 5 normal controls. Flow cytometry (CD3, 4, 8, 25 and FOXP3) was performed in 18 psoriatic patients and 8 normal volunteers and reverse transcriptase polymerase chain reaction (foxp3 mRNA) was performed in 8 psoriasis patients.
RESULTS
An increase in the FOXP3(+) cell fraction was detected in the lesional psoriatic skin irrespective of the severity of psoriasis as compared with the normal skin. However, a decrease in FOXP3(+) cells was observed in the samples obtained from psoriasis of 'acute course'. FOXP3(+) Treg populations in the blood of the 'acute course' psoriasis was not different compared to that of 'chronic course' psoriasis and normal controls.
CONCLUSION
The deficiency of FOXP3(+) Tregs in the lesional psoriatic skin might be responsible for the exacerbation of psoriasis.
MeSH Terms
Figure
-
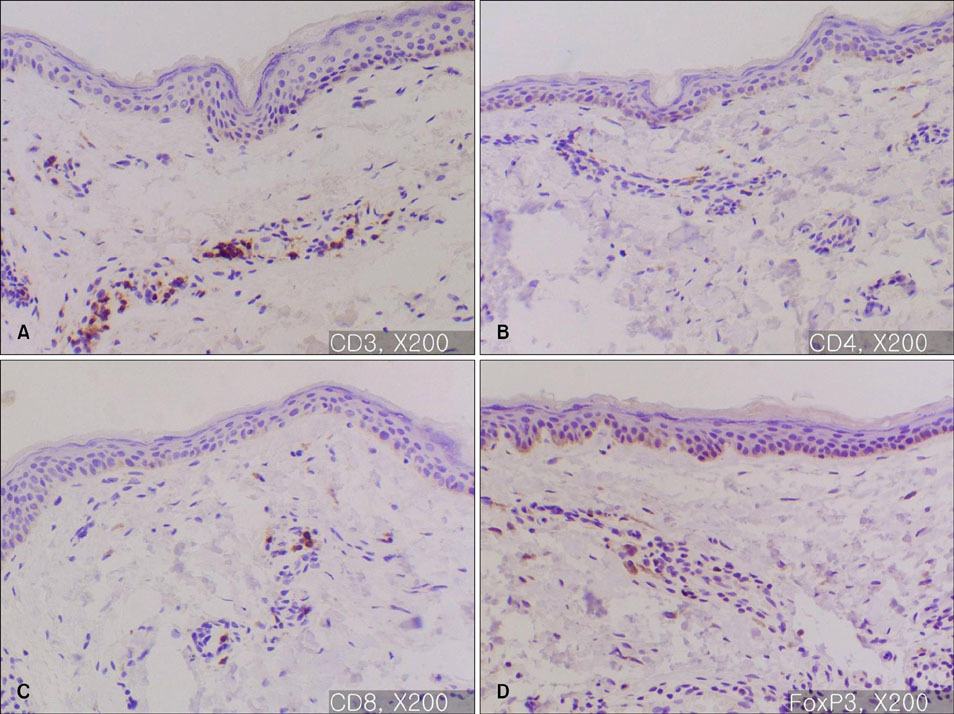
Fig. 1 Immunohistochemistry of normal skin (A: CD3, ×200, B: CD4, ×200, C: CD8, ×200, D: FOXP3, ×200). The percentage of FOXP3+ mononuclear cells in normal skin is 10~20%; the mononuclear cells are CD3, CD4 and CD8+.

Fig. 2 (A) Immunohistochemistry for FOXP3, ×200: Typical plaque type psoriasis (Case No. 3). In psoriatic skin lesions, FOXP3+ cells are mainly observed in papillary dermis, consisting of about 20~40% of the mononuclear cellular infiltration. (B) Immunohistochemistry for FOXP3, ×200: Palmoplantar pustular psoriasis (Case No. 15). FOXP3+ cells consists of about 20~30% of the mononuclear cellular infiltration.
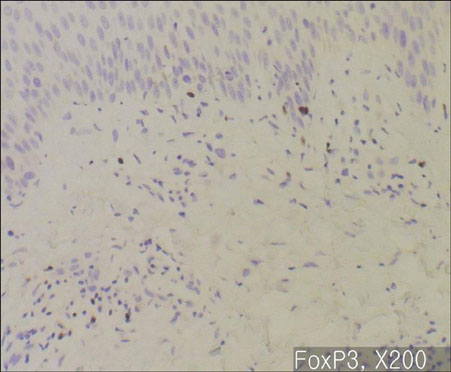
Fig. 3 Immunohistochemistry for FOXP3, ×200: Acute severe plaque type psoriasis (Case No. 4). FOXP3+ T cells are relatively deficient.

Fig. 4 Immunohistochemistry for FOXP3, ×200: Acute moderate to severe plaque type psoriasis (Case No. 8). The ratio of FOXP3+ Treg to mononuclear cells is decreased.
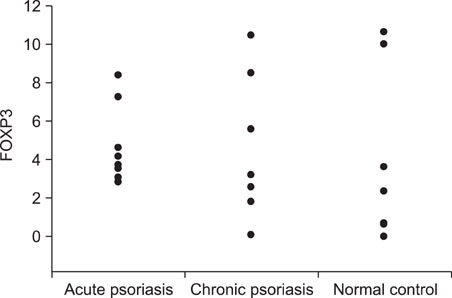
Fig. 5 Immunohistochemistry for FOXP3, ×200: Acute exacerbating erythrodermic psoriasis (Case No. 18). FOXP3+ cells are almost absent.

Fig. 6 Result of flow-cytometry for FOXP3. In all samples, the percentage of FOXP3+ was 3~10% among the peripheral blood mononuclear cells of the normal control group (n=8) and the results were similar between the cases of acute psoriasis (n=6), and chronic psoriasis (n=12).

Fig. 7 Results of flow-cytometry for CD4 and CD25. CD4+CD25high+cell fraction ranged between 3~10% of the peripheral blood mononuclear cell in all subsets of the patients.
Reference
-
1. Read S, Malmström V, Powrie F. Cytotoxic T lymphocyte-associated antigen 4 plays an essential role in the function of CD25(+)CD4(+) regulatory cells that control intestinal inflammation. J Exp Med. 2000. 192:295–302.
Article2. Shimizu J, Yamazaki S, Takahashi T, Ishida Y, Sakaguchi S. Stimulation of CD25(+)CD4(+) regulatory T cells through GITR breaks immunological self-tolerance. Nat Immunol. 2002. 3:135–142.
Article3. McHugh RS, Whitters MJ, Piccirillo CA, Young DA, Shevach EM, Collins M, et al. CD4(+)CD25(+) immunoregulatory T cells: gene expression analysis reveals a functional role for the glucocorticoid-induced TNF receptor. Immunity. 2002. 16:311–323.4. Lehmann J, Huehn J, de la Rosa M, Maszyna F, Kretschmer U, Krenn V, et al. Expression of the integrin alpha Ebeta 7 identifies unique subsets of CD25+ as well as CD25-regulatory T cells. Proc Natl Acad Sci U S A. 2002. 99:13031–13036.
Article5. Liu H, Leung BP. CD4+CD25+ regulatory T cells in health and disease. Clin Exp Pharmacol Physiol. 2006. 33:519–524.
Article6. Taams L, Vukmanovic-Stejic M, Salmon M, Akbar A. Immune regulation by CD4+CD25+ regulatory T cells: implications for transplantation tolerance. Transpl Immunol. 2003. 11:277–285.
Article7. Mutis T, Aarts-Riemens T, Verdonck LF. The association of CD25 expression on donor CD8+ and CD4+ T cells with graft-versus-host disease after donor lymphocyte infusions. Haematologica. 2005. 90:1389–1395.8. Zorn E, Kim HT, Lee SJ, Floyd BH, Litsa D, Arumugarajah S, et al. Reduced frequency of FOXP3+ CD4+CD25+ regulatory T cells in patients with chronic graft-versus-host disease. Blood. 2005. 106:2903–2911.
Article9. Liyanage UK, Moore TT, Joo HG, Tanaka Y, Herrmann V, Doherty G, et al. Prevalence of regulatory T cells is increased in peripheral blood and tumor microenvironment of patients with pancreas or breast adenocarcinoma. J Immunol. 2002. 169:2756–2761.
Article10. Woo EY, Yeh H, Chu CS, Schlienger K, Carroll RG, Riley JL, et al. Cutting edge: Regulatory T cells from lung cancer patients directly inhibit autologous T cell proliferation. J Immunol. 2002. 168:4272–4276.
Article11. Zou W. Regulatory T cells, tumour immunity and immunotherapy. Nat Rev Immunol. 2006. 6:295–307.
Article12. Kagen MH, McCormick TS, Cooper KD. Regulatory T cells in psoriasis. Ernst Schering Res Found Workshop. 2006. 193–209.
Article13. Veldman C, Nagel A, Hertl M. Type I regulatory T cells in autoimmunity and inflammatory diseases. Int Arch Allergy Immunol. 2006. 140:174–183.
Article14. Chattopadhyay S, Mehrotra S, Chhabra A, Hegde U, Mukherji B, Chakraborty NG. Effect of CD4+CD25+ and CD4+CD25- T regulatory cells on the generation of cytolytic T cell response to a self but human tumor-associated epitope in vitro. J Immunol. 2006. 176:984–990.
Article15. Chen W, Jin W, Hardegen N, Lei KJ, Li L, Marinos N, et al. Conversion of peripheral CD4+CD25- naive T cells to CD4+CD25+ regulatory T cells by TGF-beta induction of transcription factor Foxp3. J Exp Med. 2003. 198:1875–1886.
Article16. Zheng SG, Wang JH, Stohl W, Kim KS, Gray JD, Horwitz DA. TGF-beta requires CTLA-4 early after T cell activation to induce FoxP3 and generate adaptive CD4+CD25+ regulatory cells. J Immunol. 2006. 176:3321–3329.
Article17. Vissers WH, Arndtz CH, Muys L, Van Erp PE, de Jong EM, van de Kerkhof PC. Memory effector (CD45RO+) and cytotoxic (CD8+) T cells appear early in the margin zone of spreading psoriatic lesions in contrast to cells expressing natural killer receptors, which appear late. Br J Dermatol. 2004. 150:852–859.
Article18. Sugiyama H, Gyulai R, Toichi E, Garaczi E, Shimada S, Stevens SR, et al. Dysfunctional blood and target tissue CD4+CD25high regulatory T cells in psoriasis: mechanism underlying unrestrained pathogenic effector T cell proliferation. J Immunol. 2005. 174:164–173.
Article19. Bovenschen HJ, van Vlijmen-Willems IM, van de Kerkhof PC, van Erp PE. Identification of lesional CD4+ CD25+ Foxp3+ regulatory T cells in Psoriasis. Dermatology. 2006. 213:111–117.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Study on the Number of Circulating CD4+CD25+Foxp3+ Regulatory T Cells and CD4+CD25-Foxp3+ T Cells in Psoriasis
- Peripheral Generation of CD4+ CD25+ Foxp3+ Regulatory T Cells
- Dynamic Frequency of Blood CD4+CD25+ Regulatory T Cells in Rats with Collagen-induced Arthritis
- Alteration of CD4+CD25+Foxp3+ T cell level in Kawasaki disease
- Characterization of regulatory T cells in ex vivo expansion of human umbilical cord blood
