The Efficacy, Longevity, and Safety of Combined Radiofrequency Treatment and Hyaluronic Acid Filler for Skin Rejuvenation
- Affiliations
-
- 1Aesthetic Research Team, Amore Pacific Corporation Research and Development Center, Yongin, Korea.
- 2Department of Dermatology, Chung-Ang University College of Medicine, Seoul, Korea. beomjoon@unitel.co.kr
- KMID: 2265584
- DOI: http://doi.org/10.5021/ad.2014.26.4.447
Abstract
- BACKGROUND
Recent advances in hyaluronic acid (HA) fillers and radiofrequency (RF) devices have been made in the context of skin rejuvenation and cosmetic surgery. Moreover, combination regimens with both techniques are currently being developed.
OBJECTIVE
The present study was designed to examine the clinical and histologic effects of a new needle that incorporates an RF device for HA injections.
METHODS
A new intradermal needle RF device (INNOfill; Pacific Pharma, Korea) was assessed in the present study. In the animal arm, procollagen production was measured by using enzyme-linked immunosorbent assay, the filler volume was quantified by incorporating a dye with filler, and the filler distribution was assessed through the changes in tissue structure. In the human arm, the efficacy of the combination regimen was assessed by using the wrinkle severity rating scale (WSRS).
RESULTS
In the animal study, RF treatment increased procollagen production in a time-dependent fashion. The total volume was significantly increased with the RF treatment when compared with the filler injections alone, and lasted for up to 7 weeks after treatment. Additionally, the filler distribution was reduced in animals treated with RF when compared with the untreated group. In the human study, the nasolabial folds of subjects treated with RF before filler injections exhibited a significantly greater change in the WSRS score from baseline when compared with the nasolabial folds treated with filler injections alone.
CONCLUSION
A new device incorporating RF treatment before HA filler injection may represent a biocompatible and long-lasting advance in skin rejuvenation.
Keyword
MeSH Terms
Figure
-
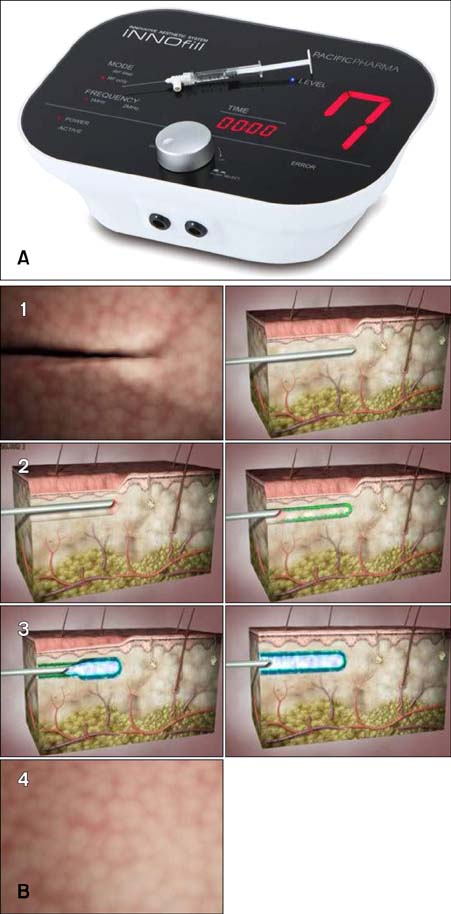
Fig. 1 (A) Novel minimally invasive radiofrequency (RF) device. (B) Procedure protocol. 1. Insertion of the needle along the wrinkle course at variable depths from the superficial to mid dermis, depending on the wrinkle type and the filler used. 2. In situ 360-degree rotation (tunneling) performed to create a virtual canal contextually supplying the RF. 3. The procedure is repeated in retrograde through a multi-prick technique along the wrinkle course. 4. Without removing the needle from the injection site, the needle retraces the course, releasing hyaluronic acid through the linear retrograde technique. This technique yields wrinkle smoothing with a long-lasting effect.
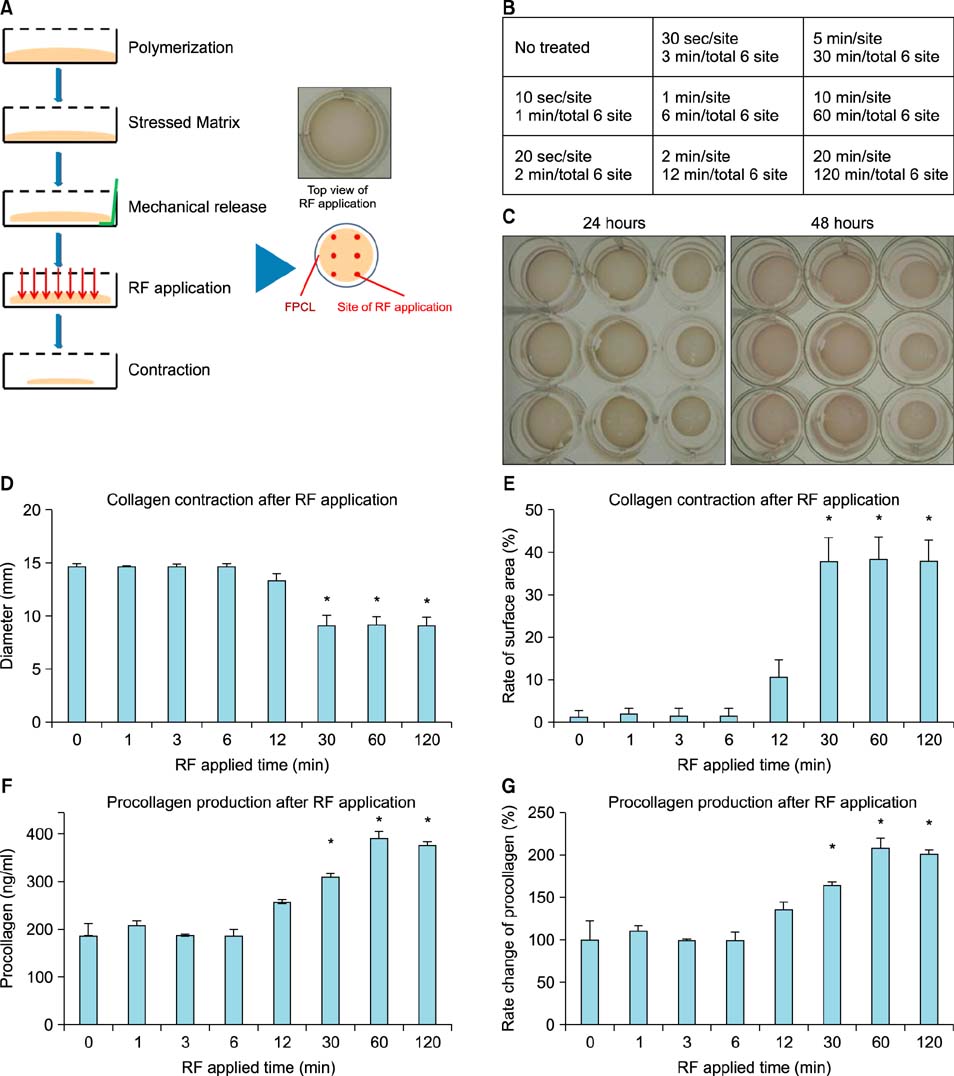
Fig. 2 Radiofrequency (RF)-induced collagen contraction and production in fibroblast-populated collagen lattices (FPCLs). (A) FPCL contraction assay diagram. As illustrated, cell-seeded matrices develop isometric tension during an initial attachment period (1~2 days) that later dissipates when lattices are mechanically released. RF treatment performed at six sites on the FPCLs after mechanical release. (B) Plate map of the RF application sites on the FPCLs. At each site, RF was delivered for 1 to 20 minutes per site in a time-dependent manner. (C) Digital images of the contracting FPCLs were captured at 24 h and 48 h after RF application. (D) FPCL contraction diameters after an incubation period of 2 days. All plotted data represent the mean±standard error of the mean (SEM) values for all three FPCLs. Statistical pairwise comparisons were performed by using Student's t-test. Statistical significance (p<0.05) was reached between normal and RF-treated FPCLs. (E) Percent change of FPCL surface area after RF treatment and an incubation period of 2 days. All plotted data represent the mean±SEM values for all three FPCLs. Statistical pairwise comparisons were performed by using Student's t-test. Statistical significance (p<0.05) was reached between normal and RF-treated FPCLs. (F, G) Procollagen production after RF treatment and an incubation period of 2 days. All plotted data represent the mean±SEM values for all three FPCLs. Statistical pairwise comparisons were performed by using Student's t-test. Statistical significance (p<0.05) was reached between normal and RF treated FPCLs. *p<0.05: significant.
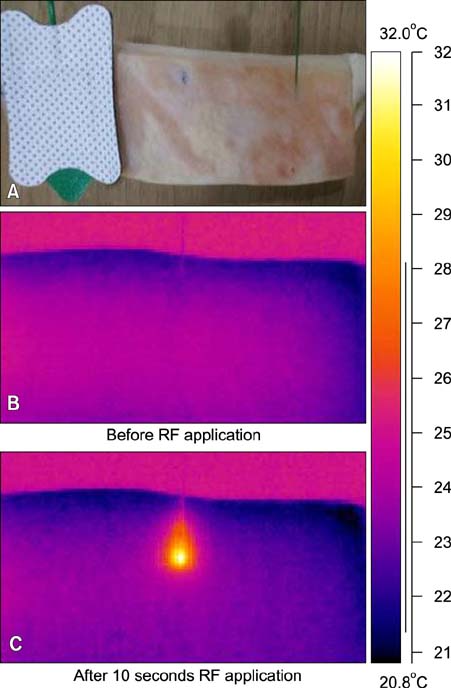
Fig. 3 (A) Thermal profiles after radiofrequency (RF) application in ex vivo porcine skin. Thermal profiles before (B) and 10 seconds after RF application (C).
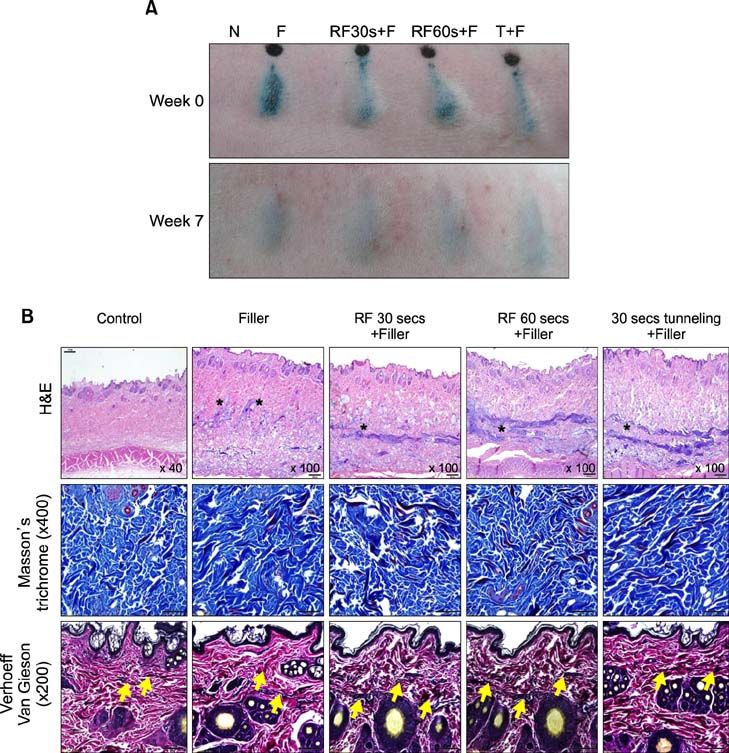
Fig. 4 (A) Volumizing effect from filler injections after radiofrequency (RF) treatment. N: normal, F: filler (Glytone 3) injection, RF30s+F: filler injection immediately after 30 seconds of RF treatment through the tunneling method, RF60s+F: filler injection immediately after 60 seconds of RF treatment through the tunneling method, T30s+F: filler injection immediately after 30 seconds of tunneling without RF treatment. (B) Filler-injected areas are shown without RF or with RF treatment ('*' sign). The filler-injected areas showed small filler particles spread in the dermis, and areas injected with filler after RF or with tunneling showed linear filler distribution in the mid or lower dermis, respectively ('*' sign). The periphery and area around the filler after RF treatment were stained with Masson's trichrome to identify the extracellular matrix components, in particular the dermal collagen. A significantly greater increase in collagen bundles was observed in subjects treated with both filler and RF when compared with those treated with filler alone (blue). Additionally, fibroplasia (red) was also observed in larger quantities after RF treatment when compared with filler injections alone. The tissue specimens were also stained with Verhoeff-Van Gieson to assess the quantity of elastin fibers in the dermis. Classically, long, thin elastin fibers are distributed throughout the papillary and upper reticular dermis. In the results presented here, a change in elastin fiber quality was observed after treatment with RF, with the elastin fibers in the papillary and reticular dermis noted to be markedly shorter ('arrow' sign).

Fig. 5 (A) Photographs of the nasolabial wrinkles of the patients at baseline and at 1, 4, 8, and 12 weeks after either filler injection or filler injection with radiofrequency treatment (RF+filler). (B) Relative wrinkle severity rating scale (WSRS) score at baseline and at 1, 4, 8, and 12 weeks after either filler injection or RF+filler treatment. All plotted data represent the mean±standard error of the mean values for the two patients. Statistical pairwise comparisons were performed by using Student's t-test. Statistical significance was reached (p<0.05) between filler and RF+filler. *p<0.05: significant. (C) Evaluation of collagen production at filler injection sites at 12 weeks.
Cited by 2 articles
-
A Randomized, Evaluator-Blinded, Split-Face Comparison Study of the Efficacy and Safety of a Novel Mannitol Containing Monophasic Hyaluronic Acid Dermal Filler for the Treatment of Moderate to Severe Nasolabial Folds
Byung Wook Kim, Ik Jun Moon, Woo Jin Yun, Bo Young Chung, Sang Duck Kim, Ga-Young Lee, Sung Eun Chang
Ann Dermatol. 2016;28(3):297-303. doi: 10.5021/ad.2016.28.3.297.Usefulness of Monopolar Thermal Radiofrequency Treatment for Periorbital Wrinkles
Song Hee Han, Yeong Min Yoon, Yang Won Lee, Yong Beom Choe, Kyu Joong Ahn
Ann Dermatol. 2018;30(3):296-303. doi: 10.5021/ad.2018.30.3.296.
Reference
-
1. El-Domyati M, Attia S, Saleh F, Brown D, Birk DE, Gasparro F, et al. Intrinsic aging vs. photoaging: a comparative histopathological, immunohistochemical, and ultrastructural study of skin. Exp Dermatol. 2002; 11:398–405.
Article2. el-Domyati M, el-Ammawi TS, Medhat W, Moawad O, Brennan D, Mahoney MG, et al. Radiofrequency facial rejuvenation: evidence-based effect. J Am Acad Dermatol. 2011; 64:524–535.
Article3. Goldman MP, Alster TS, Weiss R. A randomized trial to determine the influence of laser therapy, monopolar radiofrequency treatment, and intense pulsed light therapy administered immediately after hyaluronic acid gel implantation. Dermatol Surg. 2007; 33:535–542.
Article4. Buck DW 2nd, Alam M, Kim JY. Injectable fillers for facial rejuvenation: a review. J Plast Reconstr Aesthet Surg. 2009; 62:11–18.
Article5. Beasley KL, Weiss MA, Weiss RA. Hyaluronic acid fillers: a comprehensive review. Facial Plast Surg. 2009; 25:86–94.
Article6. Hantash BM, Ubeid AA, Chang H, Kafi R, Renton B. Bipolar fractional radiofrequency treatment induces neoelastogenesis and neocollagenesis. Lasers Surg Med. 2009; 41:1–9.
Article7. Day DJ, Littler CM, Swift RW, Gottlieb S. The wrinkle severity rating scale: a validation study. Am J Clin Dermatol. 2004; 5:49–52.8. Kim KH, Geronemus RG. Nonablative laser and light therapies for skin rejuvenation. Arch Facial Plast Surg. 2004; 6:398–409.
Article9. England LJ, Tan MH, Shumaker PR, Egbert BM, Pittelko K, Orentreich D, et al. Effects of monopolar radiofrequency treatment over soft-tissue fillers in an animal model. Lasers Surg Med. 2005; 37:356–365.
Article10. Shumaker PR, England LJ, Dover JS, Ross EV, Harford R, Derienzo D, et al. Effect of monopolar radiofrequency treatment over soft-tissue fillers in an animal model: part 2. Lasers Surg Med. 2006; 38:211–217.
Article11. Alam M, Levy R, Pajvani U, Ramierez JA, Guitart J, Veen H, et al. Safety of radiofrequency treatment over human skin previously injected with medium-term injectable soft-tissue augmentation materials: a controlled pilot trial. Lasers Surg Med. 2006; 38:205–210.
Article12. Park KY, Park MK, Li K, Seo SJ, Hong CK. Combined treatment with a nonablative infrared device and hyaluronic acid filler does not have enhanced efficacy in treating nasolabial fold wrinkles. Dermatol Surg. 2011; 37:1770–1775.
Article13. Kim JE, Sykes JM. Hyaluronic acid fillers: history and overview. Facial Plast Surg. 2011; 27:523–528.
Article14. Turlier V, Rouquier A, Black D, Josse G, Auvergnat A, Briant A, et al. Assessment of the clinical efficacy of a hyaluronic acid-based deep wrinkle filler using new instrumental methods. J Cosmet Laser Ther. 2010; 12:195–202.
Article15. Belda JI, Artola A, García-Manzanares MD, Ferrer C, Haroun HE, Hassanein A, et al. Hyaluronic acid combined with mannitol to improve protection against free-radical endothelial damage: experimental model. J Cataract Refract Surg. 2005; 31:1213–1218.
Article16. Atiyeh BS, Dibo SA. Nonsurgical nonablative treatment of aging skin: radiofrequency technologies between aggressive marketing and evidence-based efficacy. Aesthetic Plast Surg. 2009; 33:283–294.
Article17. Arnoczky SP, Aksan A. Thermal modification of connective tissues: basic science considerations and clinical implications. J Am Acad Orthop Surg. 2000; 8:305–313.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hyaluronidase: An overview of its properties, applications, and side effects
- Delayed skin discoloration spreading in the direction of gravity after injection of hyaluronic acid dermal fillers in both nasolabial folds
- A Case of Delayed Hypersensitivity Reaction due to Hyaluronic Acid (Restylane(R))
- Facial Pseudocyst Caused by Hyaluronic Acid Filler Injection: A Case Report
- Comparison of the efficacy and safety between a new monophasic hyaluronic acid filler and a biphasic hyaluronic acid filler in correcting facial wrinkles
