Ann Dermatol.
2010 Aug;22(3):370-372. 10.5021/ad.2010.22.3.370.
Cutaneous Malignant Melanoma Associated with Papillary Thyroid Cancer
- Affiliations
-
- 1Department of Dermatology, School of Medicine, Gyeongsang National University & Gyeongsang Institute of Health Science, Jinju, Korea.
- 2Department of Dermatology, School of Medicine, Kangwon National University Hospital, Chuncheon, Korea. cheewon@hotmail.com
- KMID: 2265380
- DOI: http://doi.org/10.5021/ad.2010.22.3.370
Abstract
- As the survival from cutaneous malignant melanoma and its clinical concerns have been steadily increasing, the possibility has been raised of an increased risk of second primary cancers in the patients with malignant melanoma. Especially, recent studies have identified an association between cutaneous malignant melanoma and thyroid carcinoma. We here report on a case of cutaneous malignant melanoma that developed in a 61-year-old female patient who had hypothyroidism caused by papillary thyroid carcinoma. We suggest that the individuals who have cutaneous malignant melanoma may be predisposed to other primary cancers and especially thyroid carcinoma. Continuous monitoring of the thyroid function in melanoma patients is required because hypothyroidism can worsen due to malignant melanoma and this is probably associated with thyroid carcinoma.
MeSH Terms
Figure
-

Fig. 1 The 1.0×1.0 cm sized solitary black-colored nodule with 2.5×2.0 cm sized surrounded ill-demarcated mottled patches on the left heel.

Fig. 2 (A) The histopathologic findings show scattered or nested atypical melanocytes that are arranged in a pagetoid pattern (H&E stain, ×12.5). (B) The high power view reveals nests of anaplastic epithelioid cells with melanin pigment in the tumor and dilated, enlarged vascular channels in the dermis (H&E stain, ×40).
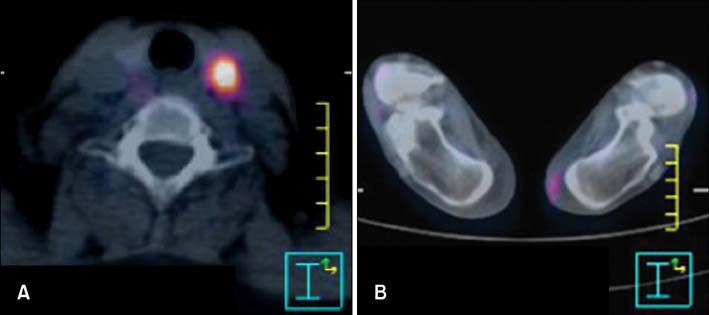
Fig. 3 The PET-CT scan finding shows focal hot lesions are checked (A) in the left lobe of the thyroid and (B) the soft tissue on the heel of the left foot.
Reference
-
1. Fraser DG, Bull JG Jr, Dunphy JE. Malignant melanoma and coexisting malignant neoplasms. Am J Surg. 1971. 122:169–174.
Article2. Shah M, Orengo IF, Rosen T. High prevalence of hypothyroidism in male patients with cutaneous melanoma. Dermatol Online J. 2006. 12:1.
Article3. Goggins W, Daniels GH, Tsao H. Elevation of thyroid cancer risk among cutaneous melanoma survivors. Int J Cancer. 2006. 118:185–188.
Article4. Kang SK, Jang AK, Choi JH, Sung KJ, Moon KC, Koh JK. Second primary cancers in patients with cutaneous malignant melanoma. Korean J Dermatol. 2001. 39:798–802.5. Ellerhorst JA, Sendi-Naderi A, Johnson MK, Cooke CP, Dang SM, Diwan AH. Human melanoma cells express functional receptors for thyroid-stimulating hormone. Endocr Relat Cancer. 2006. 13:1269–1277.
Article6. Ellerhorst JA, Naderi AA, Johnson MK, Pelletier P, Prieto VG, Diwan AH, et al. Expression of thyrotropin-releasing hormone by human melanoma and nevi. Clin Cancer Res. 2004. 10:5531–5536.
Article7. Soares P, Trovisco V, Rocha AS, Lima J, Castro P, Preto A, et al. BRAF mutations and RET/PTC rearrangements are alternative events in the etiopathogenesis of PTC. Oncogene. 2003. 22:4578–4580.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Metastatic Melanoma Mimicking a Papillary Carcinoma of the Thyroid in Fine Needle Aspiration Cytology: A Case Report
- Four Cases of Malignant Pleural Effusion in Patients with Papillary Thyroid Carcinoma
- Multiple metastasis of follicular variant of papillary thyroid carcinoma coexistent with malignant melanoma
- Three Cases of Malignant Melanoma Possibly Arising in a Long Standing Melanocytic Nevus
- Second Primary Cancers in Patients with Cutaneous Malignant Melanoma
