Surgical anatomy of the upper eyelid relating to upper blepharoplasty or blepharoptosis surgery
- Affiliations
-
- 1Department of Plastic Surgery and Center for Advanced Medical Education by BK21 Project, Inha University School of Medicine, Incheon, Korea. jokerhg@inha.ac.kr
- KMID: 2263101
- DOI: http://doi.org/10.5115/acb.2013.46.2.93
Abstract
- Eyelid anatomy, including thickness measurements, was examined in numerous age groups. The thickest part of the upper eyelid is just below the eyebrow (1.127+/-238 microm), and the thinnest near the ciliary margin (320+/-49 microm). The thickness of skin at 7 mm above the eyelashes was 860+/-305 microm. The results revealed no significant differences among the age groups. Fast fibers (87.8+/-3.7%) occupied a significantly larger portion of the orbicularis oculi muscle (OOM) than nonfast fibers (12.2+/-3.7%). The frontalis muscle passed through and was inserted into the bundles of the OOM on the superior border of the eyebrow at the middle and medial portions of the upper eyelid. Laterally, the frontalis muscle inserted about 0.5 cm below the superior border of the eyebrow. Fast fibers occupied a significantly larger portion of the OOM than did non-fast fibers. The oculomotor nerve ends that extend forward to the distal third of the levator muscle are exposed and vulnerable to local anesthetics and may be numbed during blepharoplasty. The orbital septum consists of 2 layers. The outer layer of loose connective tissue descends to interdigitate with the levator aponeurosis and disperses inferiorly. The inner layer follows the outer layer, then reflects and continues posteriorly with the levator sheath. Widths of the tarsal plate at its lower border, mid-height, and upper border were 21.8+/-1.8, 16.2+/-1.6, and 8.3+/-1.0 mm, respectively. The widths of the levator aponeurosis were 32.0+/-2.2, 29.2+/-3.5, and 27.2+/-3.9 mm, respectively. Below the levator, the "conjoint fascial sheath" (CFS) is attached to the conjunctival fornix. The CFS was 12.2+/-2.0 mm anteroposterior length and 1.1+/-0.1 mm thick. The shape was equilateral trapezoid with a longer base anteriorly. The superior palpebral muscle was trapezoidal. The lengths of its sides were 15.58+/-1.82 and 22.30+/-5.25 mm, and its height was 13.70+/-2.74 mm. The width of the levator aponeurosis was approximately 4 mm wider than the superior palpebral muscle.
Keyword
MeSH Terms
Figure
-
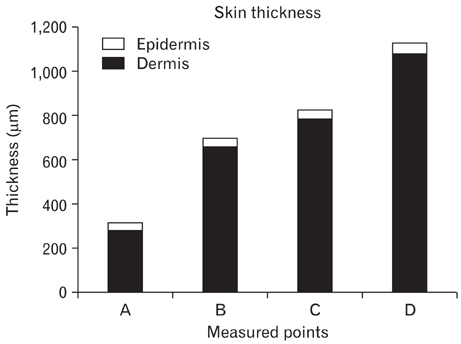
Fig. 1 Histograms showing epidermis and dermis thickness as measured at various points. A, near the ciliary margin; B, midtarsus; C, upper tarsal border; D, lower border of the eyebrow.
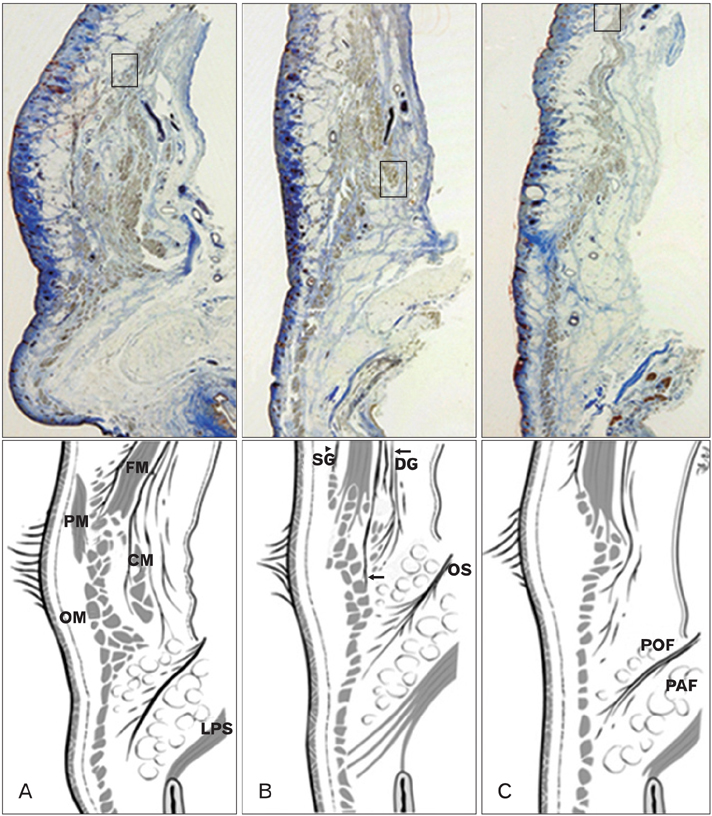
Fig. 2 Sagittal sections of the upper eyelid. The anterior surface of the frontalis muscle is enveloped by superficial galea (SG, arrowhead) and deep galea (DG, arrows) on its posterior surface. The frontalis muscle (FM) passes through and inserts in the bundles of the orbicularis oculi muscle (OM). (A) Medial section. The FM inserts in the superior border of the eyebrow. The most distal part of the FM is located deep to the procerus muscle (PM) and superficial to the corrugator muscle (CM). (B) Middle section. The FM inserts in the superior border of the eyebrow. (C) Lateral section (the FM inserts about 0.5 cm below the superior border of the eyebrow). OS, orbital septum; PAF, pre-aponeurotic fat; POF, pre-orbicularis fascia.

Fig. 3 Schema of a sagittal section of the eyelid. Reproduced from Whitnall SE. J Anat Physiol 1911;45:131-9 [21], with permission from John Wiley & Sons Ltd. Sept. ort, septum orbitale; Palp. aporn, palpebral aponeurosis.

Fig. 4 Schema of the levator aponeurosis (black trapezoid) and tarsal plate (T, gray trapezoid). Upper: Levator aponeurosis width was measured at the lower border, mid-region, and upper border of the tarsal plate to be 32.0±2.2 mm, 29.2±3.5 mm, 27.2±3.9 mm, respectively. Lower: The medial brim of the levator aponeurosis at the lower border, mid-region, and upper border of the tarsal plate was 3.6±1.1 mm, 5.1±1.0 mm, and 6.2±1.1 mm, respectively. The lateral brim of the levator aponeurosis at the lower border, mid-region, and upper border of the tarsal plate was 6.6±0.9 mm, 7.9±2.6 mm, and 12.7±3.7 mm, respectively. N, nasal side; W, superior transverse ligament of Whitnall.

Fig. 5 Microscopic findings of the upper eyelid. (A, B) Through the medial limbus line, (C, D) midpupillary line, (E, F) through the lateral limbus line. The conjoint fascial sheath (CFS) was located in the intermuscular space between the anterior third of the superior rectus (S) and the levator (L). Posteriorly, it extended from the fascia of the levator and superior rectus. Anteriorly, superficial and deep extensions (arrows) of CFS continued approximately 2 mm to the superior conjunctival fornix and then 2-3 mm distally (arrowheads) along and beneath the palpebral and bulbar conjunctiva. A, levator aponeurosis; F, pre-aponeurotic fat; LG, lacrimal gland; O, orbicularis oculi muscle; OS, orbital septum; SO, superior oblique; W, Whitnall's superior transverse ligament. Scale bar in (E)=2 mm (A-F).

Fig. 6 Schema of a parasagittal section through the midpupillary line. The levator palpebrae superior muscle divides into superficial (S) and deep (D) parts beneath the superior transverse ligament. The levator aponeurosis originates from this superficial portion. The superior palpebral muscle originates from the deep portion. A, levator aponeurosis; M, superior palpebral involuntary muscle (Müller's muscle); LP, levator palpebrae muscle; SR, superior rectus muscle.

Fig. 7 Schema of the superior palpebral muscle (M) and levator aponeurosis. (A) The width of the superior palpebral muscle was 15.6 mm at the anterior border of the superior transverse ligament and 22.3 mm at the upper border of the tarsal plate. The height was 13.7 mm. (B) The width of the levator aponeurosis was wider than that of the superior palpebral muscle. The width of the levator aponeurosis was 19.3 mm at the anterior border of the superior transverse ligament and 26.8 mm at the upper border of the tarsal plate. Medially, the levator aponeurosis was 1.9 and 1.6 mm wider at the level of the superior transverse ligament and the upper tarsal border, respectively. Laterally, the levator aponeurosis was 1.8 and 1.6 mm wider at the level of the superior transverse ligament and at the upper tarsal border, respectively. LP, levator palpebrae muscle.
Cited by 1 articles
-
Changes in the Horizontal Angular Direction of Lower Eyelashes with Age in Korean Patients
Jungah Huh, Jinhwan Park, Sehyun Baek
J Korean Ophthalmol Soc. 2018;59(2):105-109. doi: 10.3341/jkos.2018.59.2.105.
Reference
-
1. Barker DE. Skin thickness in the human. Plast Reconstr Surg (1946). 1951. 7:115–116.2. Lee Y, Hwang K. Skin thickness of Korean adults. Surg Radiol Anat. 2002. 24:183–189.3. Hwang K, Kim DJ, Hwang SH. Thickness of Korean upper eyelid skin at different levels. J Craniofac Surg. 2006. 17:54–56.4. Gonzalez-Ulloa M, Flores ES. Senility of the face: basic study to understand its causes and effects. Plast Reconstr Surg. 1965. 36:239–246.5. Hykin PG, Bron AJ. Age-related morphological changes in lid margin and meibomian gland anatomy. Cornea. 1992. 11:334–342.6. Hwang K, Kim DJ, Kim SK. Does the upper eyelid skin become thinner with age? J Craniofac Surg. 2006. 17:474–476.7. Lipham WJ, Tawfik HA, Dutton JJ. A histologic analysis and three-dimensional reconstruction of the muscle of Riolan. Ophthal Plast Reconstr Surg. 2002. 18:93–98.8. Sullivan L. Form follows function [Internet]. cited 2010 Dec 15. Wikipedia;Available from: http://en.wikipedia.org/wiki/Form_follows_function.9. McLoon LK, Wirtschafter JD. Regional differences in the orbicularis oculi muscle: conservation between species. J Neurol Sci. 1991. 104:197–202.10. Goodmurphy CW, Ovalle WK. Morphological study of two human facial muscles: orbicularis oculi and corrugator supercilii. Clin Anat. 1999. 12:1–11.11. Hwang K, Huan F, Kim DJ. Muscle fiber types of human orbicularis oculi muscle. J Craniofac Surg. 2011. 22:1827–1830.12. Hwang K, Kim DJ, Hwang SH. Immunohistochemical study of differences between the muscle fiber types in the pars peripheralis and marginalis. J Craniofac Surg. 2007. 18:591–593.13. Standring S. Gray's anatomy: the anatomical basis of clinical practice. 2005. 39th ed. Edinburgh: Elsevier;500–501. 69114. Ramirez OM, Peña G. Frontalis muscle advancement: a dynamic structure for the treatment of severe congenital eyelid ptosis. Plast Reconstr Surg. 2004. 113:1841–1849.15. Knize DM. An anatomically based study of the mechanism of eyebrow ptosis. Plast Reconstr Surg. 1996. 97:1321–1333.16. Karacalar A, Korkmaz A, Kale A, Kopuz C. Compensatory brow asymmetry: anatomic study and clinical experience. Aesthetic Plast Surg. 2005. 29:119–123.17. Hwang K, Kim DJ, Hwang SH. Insertion of frontalis muscle relating to blepharoptosis repair. J Craniofac Surg. 2005. 16:965–967.18. Rainin EA, Carlson BM. Postoperative diplopia and ptosis. A clinical hypothesis based on the myotoxicity of local anesthetics. Arch Ophthalmol. 1985. 103:1337–1339.19. Kalichman MW. Physiologic mechanisms by which local anesthetics may cause injury to nerve and spinal cord. Reg Anesth. 1993. 18:6 Suppl. 448–452.20. Hwang K, Lee DK, Chung IH, Lee SI. Patterns of oculomotor nerve distribution to the levator palpebrae superioris muscle, and correlation to temporary ptosis after blepharoplasty. Ann Plast Surg. 2001. 47:381–384.21. Whitnall SE. A ligament acting as a check to the action of the levator palpebrae superioris muscle. J Anat Physiol. 1911. 45(Pt 2):131–139.22. Hwang K, Kim DJ, Chung RS, Lee SI, Hiraga Y. An anatomical study of the junction of the orbital septum and the levator aponeurosis in Orientals. Br J Plast Surg. 1998. 51:594–598.23. Bron AJ, Tripathi RC, Tripathi BJ. Wolff's anatomy of the eye and orbit. 1997. 8th ed. London: Arnold;14145–146.24. Werb A. Senile ptosis. Trans Ophthalmol Soc U K. 1985. 104(Pt 1):22–25.25. Hwang K, Kim DJ, Huan F, Han SH, Hwang SW. Width of the levator aponeurosis is broader than the tarsal plate. J Craniofac Surg. 2011. 22:1061–1063.26. Lockwood CB. The anatomy of the muscles, ligaments, and fasclae of the orbit, including an account of the capsule of tenon, the check ligaments of the recti, and the suspensory ligaments of the eye. J Anat Physiol. 1885. 20(Pt 1):i2–i25.27. Toldt C, Rosa AD, Paul E. An atlas human anatomy for students and physicians. 6th section. 1904. London: Rebman Limited;956u–956v.28. Whitnall SE. The levator palpebrae superioris muscle: the attachments and relations of its aponeurosis. Ophthalmoscope. 1914. 12:258–263.29. Whitnall SE. The anatomy of the human orbit and accessory organs of vision. 1932. 2nd ed. London: Humphrey Milford;141–146.30. Fink WH. An anatomic study of the check mechanism of the vertical muscles of the eyes. Am J Ophthalmol. 1957. 44:800–809.31. Manson PN, Clifford CM, Su CT, Iliff NT, Morgan R. Mechanisms of global support and posttraumatic enophthalmos: I. The anatomy of the ligament sling and its relation to intramuscular cone orbital fat. Plast Reconstr Surg. 1986. 77:193–202.32. Ettl A, Priglinger S, Kramer J, Koornneef L. Functional anatomy of the levator palpebrae superioris muscle and its connective tissue system. Br J Ophthalmol. 1996. 80:702–707.33. Holmstrom H, Santanelli F. Suspension of the eyelid to the check ligament of the superior fornix for congenital blepharoptosis. Scand J Plast Reconstr Surg Hand Surg. 2002. 36:149–156.34. Holmström H, Bernström-Lundberg C, Oldfors A. Anatomical study of the structures at the roof of the orbit with special reference to the check ligament of the superior fornix. Scand J Plast Reconstr Surg Hand Surg. 2002. 36:157–159.35. Hwang K, Shin YH, Kim DJ. Conjoint fascial sheath of the levator and superior rectus attached to the conjunctival fornix. J Craniofac Surg. 2008. 19:241–245.36. Duke-Elder S, Wybar KC. The anatomy of the visual system. System of ophthalmology. 1961. Vol. 2. St Louis: CV Mosby;446–447.37. Isaksson I. Studies on congenital genuine blepharoptosis. Morphological and functional investigations of the upper eyelid. Acta Ophthalmol Suppl. 1962. 72:1–121.38. Hwang K, Huan F, Kim DJ, Hwang SH. Size of the superior palpebral involuntary muscle (Müller muscle). J Craniofac Surg. 2010. 21:1626–1629.39. Collin JR, Beard C, Wood I. Experimental and clinical data on the insertion of the levator palpebrae superioris muscle. Am J Ophthalmol. 1978. 85:792–801.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Upper Eyelid Blepharoplasty in Aged Persons
- Correction of the Sunken Upper Eyelid Depending on the Dermatochalasis or Blepharoptosis Using the Autologous Fat Grafting
- Tarsal Margin Rotation with Blepharoplasty to Correct Cicatricial Entropion of The Upper Eyelid
- Acquired Simulated Brown Syndrome Combined with Blepharoptosis after Upper Blepharoplasty
- Key Words: Blepharoptosis, Pterigium excision, Eyelid speculum Correction Cases of Blepharoptosis Following Pterygium Excision
