Allergy Asthma Respir Dis.
2013 Mar;1(1):60-66. 10.4168/aard.2013.1.1.60.
Forced expiratory flow between 25% and 75% of vital capacity as a predictor for bronchial hyperresponsiveness in children with allergic rhinitis
- Affiliations
-
- 1Department of Pediatrics, Institute of Allergy, Yonsei University College of Medicine, Seoul, Korea. mhsohn@yuhs.ac
- KMID: 2263061
- DOI: http://doi.org/10.4168/aard.2013.1.1.60
Abstract
- PURPOSE
Allergic rhinitis (AR) is regarded as a risk factor for asthma and bronchial hyperresponsiveness (BHR) is frequently observed in patients with AR. The purpose of this study is to analyze the characteristics of AR patients with BHR and identify factors that contribute to the incidence of BHR.
METHODS
The medical records of a total of 176 children with AR were analyzed retrospectively. All patients were evaluated by performing spirometry and a methacholine challenge test.
RESULTS
One hundred and fifty-five patients (88%) were classified as the BHR-negative group and 21 patients (12%) were classified as the BHR-positive group. Forced expiratory flow between 25% and 75% of vital capacity (FEF25-75 %predicted) was reduced, and total eosinphil counts, total immunoglobulin E (IgE) level, and serum specific IgE levels of Dermatophagoides pteronyssinus and Dermatophagoides farinae were higher in the BHR-positive group compared to the BHR-negative group. However, FEF25-75 was the only statistically significant predictor for the presence of BHR on multivariate logistic regression analysis. The cutoff value to distinguish BHR-positive subjects obtained from a receiver operating characteristics curve of FEF25-75 was 88.4%. A higher frequency of BHR was found in the group with a FEF25-75 less than 88.4%, and the sensitivity, specificity, positive predictive value and negative predictive value were 57.1%, 80.6%, 28.6%, and 93.3%, respectively.
CONCLUSION
Reduced FEF25-75 values in children with AR can be helpful in predicting BHR. Children with low FEF25-75 in spirometric tests should be followed closely for apparent onset of clinical symptoms of asthma.
MeSH Terms
-
Asthma
Child
Dermatophagoides farinae
Dermatophagoides pteronyssinus
Humans
Immunoglobulin E
Immunoglobulins
Incidence
Logistic Models
Medical Records
Methacholine Chloride
Retrospective Studies
Rhinitis
Rhinitis, Allergic, Perennial
Risk Factors
ROC Curve
Spirometry
Vital Capacity
Immunoglobulin E
Immunoglobulins
Methacholine Chloride
Figure
-
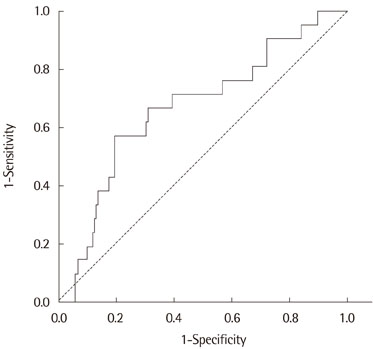
Fig. 1 Receiver operating characteristics curve of forced expiratory flow between 25% and 75% of vital capacity as a diagnostic test for bronchial hyperresponsiveness. The area under the curve was 0.669 (95% confidence interval, 0.543 to 0.794; P=0.012) and the optimal cutoff value to distinguish patients with bronchial hyperresponsiveness was 88.4%.
Cited by 1 articles
-
Research on pediatric allergic rhinitis in Korea
Kyung Suk Lee, Yeong Ho Rha
Allergy Asthma Respir Dis. 2018;6(Suppl 1):S58-S65. doi: 10.4168/aard.2018.6.S1.S58.
Reference
-
1. Christodoulopoulos P, Cameron L, Durham S, Hamid Q. Molecular pathology of allergic disease. II: Upper airway disease. J Allergy Clin Immunol. 2000. 105(2 Pt 1):211–223.2. Bousquet J, Bullinger M, Fayol C, Marquis P, Valentin B, Burtin B. Assessment of quality of life in patients with perennial allergic rhinitis with the French version of the SF-36 Health Status Questionnaire. J Allergy Clin Immunol. 1994. 94(2 Pt 1):182–188.
Article3. Ciprandi G, Cirillo I, Vizzaccaro A, Tosca M, Passalacqua G, Pallestrini E, et al. Seasonal and perennial allergic rhinitis: is this classification adherent to real life? Allergy. 2005. 60:882–887.
Article4. Bertelsen RJ, Carlsen KC, Carlsen KH. Rhinitis in children: co-morbidities and phenotypes. Pediatr Allergy Immunol. 2010. 21(4 Pt 1):612–622.
Article5. Asher I. ISAAC International Study of Asthma and Allergies in Childhood. Pediatr Pulmonol. 2007. 42:100.
Article6. Plaschke PP, Janson C, Norrman E, Bjornsson E, Ellbjar S, Jarvholm B. Onset and remission of allergic rhinitis and asthma and the relationship with atopic sensitization and smoking. Am J Respir Crit Care Med. 2000. 162(3 Pt 1):920–924.
Article7. Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy. 2008. 63:Suppl 86. 8–160.8. Suh DI, Lee JK, Lee JH, Koh YY. Bronchodilator response and its relationship to bronchial hyperresponsiveness in children with allergic rhinitis/asthma. Pediatr Allergy Respir Dis. 2010. 20:59–67.9. Wallace DV, Dykewicz MS, Bernstein DI, Blessing-Moore J, Cox L, Khan DA, et al. The diagnosis and management of rhinitis: an updated practice parameter. J Allergy Clin Immunol. 2008. 122:2 Suppl. S1–S84.
Article10. Riccio AM, Tosca MA, Cosentino C, Pallestrini E, Ameli F, Canonica GW, et al. Cytokine pattern in allergic and non-allergic chronic rhinosinusitis in asthmatic children. Clin Exp Allergy. 2002. 32:422–426.
Article11. Ciprandi G, Cirillo I, Vizzaccaro A, Milanese M, Tosca MA. Airway function and nasal inflammation in seasonal allergic rhinitis and asthma. Clin Exp Allergy. 2004. 34:891–896.
Article12. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease (COPD) and asthma. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, November 1986. Am Rev Respir Dis. 1987. 136:225–244.13. Jeffery PK, Wardlaw AJ, Nelson FC, Collins JV, Kay AB. Bronchial biopsies in asthma. An ultrastructural, quantitative study and correlation with hyperreactivity. Am Rev Respir Dis. 1989. 140:1745–1753.
Article14. Mete N, Sin A, Gulbahar O, Erdinc M, Sebik F, Kokuludag A. The determinants of bronchial hyperresponsiveness in patients with allergic rhinitis. Ann Allergy Asthma Immunol. 2004. 93:193–199.
Article15. Choi SH, Yoo Y, Yu J, Rhee CS, Min YG, Koh YY. Bronchial hyperresponsiveness in young children with allergic rhinitis and its risk factors. Allergy. 2007. 62:1051–1056.
Article16. Suh DI, Lee JK, Kim JT, Min YG, Koh YY. Bronchial hyperresponsiveness in preschool children with allergic rhinitis. Am J Rhinol Allergy. 2011. 25:e186–e190.
Article17. Ramsdale EH, Morris MM, Roberts RS, Hargreave FE. Asymptomatic bronchial hyperresponsiveness in rhinitis. J Allergy Clin Immunol. 1985. 75:573–577.
Article18. Braman SS, Barrows AA, DeCotiis BA, Settipane GA, Corrao WM. Airway hyperresponsiveness in allergic rhinitis. A risk factor for asthma. Chest. 1987. 91:671–674.19. Jang AS. Nasal eosinophilic inflammation contributes to bronchial hyperresponsiveness in patients with allergic rhinitis. J Korean Med Sci. 2002. 17:761–764.
Article20. Ciprandi G, Tosca MA, Cirillo I, Capasso M. Impact of allergic rhinitis on asthma in children: effects on bronchial hyperreactivity. Allergy. 2010. 65:1199–1201.
Article21. Cuttitta G, Cibella F, La Grutta S, Hopps MR, Bucchieri S, Passalacqua G, et al. Non-specific bronchial hyper-responsiveness in children with allergic rhinitis: relationship with the atopic status. Pediatr Allergy Immunol. 2003. 14:458–463.
Article22. Foresi A, Leone C, Pelucchi A, Mastropasqua B, Chetta A, D'Ippolito R, et al. Eosinophils, mast cells, and basophils in induced sputum from patients with seasonal allergic rhinitis and perennial asthma: relationship to methacholine responsiveness. J Allergy Clin Immunol. 1997. 100:58–64.
Article23. Ciprandi G, Tosca MA, Signori A, Cirillo I. Bronchial hyperreactivity in patients with allergic rhinitis: forced expiratory flow between 25 and 75% of vital capacity might be a predictive factor. Allergy Asthma Proc. 2011. 32:4–8.
Article24. Parker AL, Abu-Hijleh M, McCool FD. Ratio between forced expiratory flow between 25% and 75% of vital capacity and FVC is a determinant of airway reactivity and sensitivity to methacholine. Chest. 2003. 124:63–69.
Article25. Ciprandi G, Signori A, Cirillo I. Relationship between bronchial hyperreactivity and bronchodilation in patients with allergic rhinitis. Ann Allergy Asthma Immunol. 2011. 106:460–466.
Article26. Koh YY, Lee MH, Kim CK, Min YG, Kim YK, Min KU, et al. A familial predisposition in bronchial hyperresponsiveness among patients with allergic rhinitis. J Allergy Clin Immunol. 1998. 102(6 Pt 1):921–926.
Article27. American Thoracic Society. Standardization of Spirometry, 1994 Update. Am J Respir Crit Care Med. 1995. 152:1107–1136.28. Takase M, Sakata H, Shikada M, Tatara K, Fukushima T, Miyakawa T. Development of reference equations for spirometry in Japanese children aged 6-18 years. Pediatr Pulmonol. 2013. 48:35–44.
Article29. Blaiss MS. Rhinitis-asthma connection: epidemiologic and pathophysiologic basis. Allergy Asthma Proc. 2005. 26:35–40.30. Mattiello R, Mallol J, Fischer GB, Mocelin HT, Rueda B, Sarria EE. Pulmonary function in children and adolescents with postinfectious bronchiolitis obliterans. J Bras Pneumol. 2010. 36:453–459.31. Bjermer L. History and future perspectives of treating asthma as a systemic and small airways disease. Respir Med. 2001. 95:703–719.
Article32. Rao DR, Gaffin JM, Baxi SN, Sheehan WJ, Hoffman EB, Phipatanakul W. The utility of forced expiratory flow between 25% and 75% of vital capacity in predicting childhood asthma morbidity and severity. J Asthma. 2012. 49:586–592.
Article33. Ciprandi G, Cirillo I, Pistorio A. Impact of allergic rhinitis on asthma: effects on spirometric parameters. Allergy. 2008. 63:255–260.
Article34. Munoz-Lopez F, Rios-Alcolea M. The interest of FEF(25-75) in evaluating bronchial hyperresponsiveness with the methacholine test. Allergol Immunopathol (Madr). 2012. 40:352–356.
Article35. Ciprandi G, Tosca MA, Castellazzi AM, Cairello F, Salpietro C, Arrigo T, et al. FEF(25-75) might be a predictive factor for bronchial inflammation and bronchial hyperreactivity in adolescents with allergic rhinitis. Int J Immunopathol Pharmacol. 2011. 24:4 Suppl. 17–20.
Article36. Simon MR, Chinchilli VM, Phillips BR, Sorkness CA, Lemanske RF Jr, Szefler SJ, et al. Forced expiratory flow between 25% and 75% of vital capacity and FEV1/forced vital capacity ratio in relation to clinical and physiological parameters in asthmatic children with normal FEV1 values. J Allergy Clin Immunol. 2010. 126:527.e1–534.e8.
Article37. Skoner DP. Allergic rhinitis: definition, epidemiology, pathophysiology, detection, and diagnosis. J Allergy Clin Immunol. 2001. 108:1 Suppl. S2–S8.
Article38. Paoletti P, Carrozzi L, Viegi G, Modena P, Ballerin L, Di Pede F, et al. Distribution of bronchial responsiveness in a general population: effect of sex, age, smoking, and level of pulmonary function. Am J Respir Crit Care Med. 1995. 151:1770–1777.
Article39. Simons FE. Allergic rhinobronchitis: the asthma-allergic rhinitis link. J Allergy Clin Immunol. 1999. 104(3 Pt 1):534–540.
Article40. Di Lorenzo G, Mansueto P, Melluso M, Morici G, Norrito F, Esposito Pellitteri M, et al. Non-specific airway hyperresponsiveness in mono-sensitive Sicilian patients with allergic rhinitis. Its relationship to total serum IgE levels and blood eosinophils during and out of the pollen season. Clin Exp Allergy. 1997. 27:1052–1059.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Exhaled nitric oxide and bronchial hyperresponsiveness in atopic asthmatic children with and without allergic rhinitis
- Relationships of Methacholine and Adenosine 5'-Monophosphate Responsiveness with deltaFVC in Children with Allergic Rhinitis
- Usefulness of FEF25-75% in Methacholine Bronchial Provocation Test in Children with Asthma
- Pale nasal mucosa affects airflow limitations in upper and lower airways in asthmatic children
- Bronchodilator Response and Its Relationship to Bronchial Hyperresponsiveness in Children with Allergic Rhinitis/Asthma
