Allergy Asthma Immunol Res.
2011 Jan;3(1):53-57. 10.4168/aair.2011.3.1.53.
Nutritional Status According to Sensitized Food Allergens in Children With Atopic Dermatitis
- Affiliations
-
- 1Atopy Clinic, Seoul Medical Center, Seoul, Korea. hyeyung@gmail.com
- 2Atopy Research Institute, Seoul Medical Center, Seoul, Korea.
- KMID: 2260378
- DOI: http://doi.org/10.4168/aair.2011.3.1.53
Abstract
- PURPOSE
Food allergies can affect the growth and nutritional status of children with atopic dermatitis (AD). This study was conducted to determine the association between the number of sensitized food allergens and the growth and nutritional status of infants and young children with AD.
METHODS
We studied 165 children with AD, aged 5 to 47 months, and who visited the Atopy Clinic of the Seoul Medical Center. We recorded the birth weight, time at which food weaning began, scoring of atopic dermatitis (SCORAD) index, eosinophil counts in peripheral blood, and total serum IgE and specific IgE to six major allergens (egg white, cow's milk, soybean, peanut, wheat, and fish). The height and weight for age and weight for height were converted to z-scores to evaluate their effects on growth and nutritional status. Specific IgE levels > or =0.7 kUA/L, measured via the CAP assay, were considered positive.
RESULTS
As the number of sensitized food allergens increased, the mean z-scores of weight and height for age decreased (P=0.006 and 0.018, respectively). The number directly correlated with the SCORAD index (r=0.308), time at which food weaning began (r=0.332), eosinophil counts in peripheral blood (r=0.266), and total serum IgE (r=0.394). Inverse correlations were observed with the z-scores of weight for age (r=-0.358), height for age (r=-0.278), and weight for height (r=-0.224).
CONCLUSIONS
A higher number of sensitized food allergens was associated with negative effects on the growth and nutritional status of infants and young children with AD. Therefore, a thorough evaluation of both growth and nutritional status, combined with adequate patient management, is crucial in pediatric AD patients presenting with numerous sensitized food allergies.
MeSH Terms
Figure
-
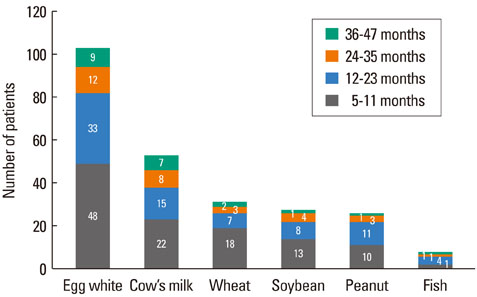
Figure Distribution of patients sensitized to food allergens.
Reference
-
1. Kim KE. Genetics of atopy and asthma. Pediatr Allergy Respir Dis. 1999. 9:343–350.2. Elliott K, Forrest S. Bieber T, Leung DYM, editors. Genetics of atopic dermatitis. Atopic dermatitis. 2002. New York: Marcel Dekker;81–110.3. Wang J, Sampson HA. Nutrition in infant allergy: a step in the right direction. Holist Nurs Pract. 2006. 20:299–302.4. Arshad SH. Food allergen avoidance in primary prevention of food allergy. Allergy. 2001. 56:Suppl 67. 113–116.5. Sicherer SH, Sampson HA. 9. Food allergy. J Allergy Clin Immunol. 2006. 117:S470–S475.6. Sicherer SH, Sampson HA. Food hypersensitivity and atopic dermatitis: pathophysiology, epidemiology, diagnosis, and management. J Allergy Clin Immunol. 1999. 104:S114–S122.7. Mofidi S. Nutritional management of pediatric food hypersensitivity. Pediatrics. 2003. 111:1645–1653.8. Fox AT, Du Toit G, Lang A, Lack G. Food allergy as a risk factor for nutritional rickets. Pediatr Allergy Immunol. 2004. 15:566–569.9. Lee DG, Rho YI, Moon KR. Assessment of nutritional status in hospitalized pediatric patients. Korean J Pediatr Gastroenterol Nutr. 2001. 4:83–91.10. Blackburn GL, Benotti PN, Bistrian BR, Bothe A, Maini BS, Schlamm HT, Smith MF. Nutritional assessment and treatment of hospital malnutrition. Infusionsther Klin Ernahr. 1979. 6:238–250.11. Kristmundsdottir F, David TJ. Growth impairment in children with atopic eczema. J R Soc Med. 1987. 80:9–12.12. Massarano AA, Hollis S, Devlin J, David TJ. Growth in atopic eczema. Arch Dis Child. 1993. 68:677–679.13. Katz KA, Mahlberg MJ, Honig PJ, Yan AC. Rice nightmare: kwashiorkor in 2 Philadelphia-area infants fed rice dream beverage. J Am Acad Dermatol. 2005. 52:S69–S72.14. Noimark L, Cox HE. Nutritional problems related to food allergy in childhood. Pediatr Allergy Immunol. 2008. 19:188–195.15. Chung SJ, Han YS, Chung SW, Ahn KM, Park HY, Lee SI, Cho YY, Choi HM. Marasmus and kwashiorkor by nutritional ignorance related to vegetarian diet and infants with atopic dermatitis in South Korea. Korean J Nutr. 2004. 37:540–549.16. Groetch M. Metcalfe DD, Sampson HA, Simon RA, editors. Diet and nutrition. Food allergy: adverse reactions to foods and food additives. 2008. 4th ed. Malden: Blackwell;482–497.17. Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol Suppl (Stockh). 1980. 92:44–47.18. Dibley MJ, Staehling N, Nieburg P, Trowbridge FL. Interpretation of Z-score anthropometric indicators derived from the international growth reference. Am J Clin Nutr. 1987. 46:749–762.19. de Onis M, Blossner M. WHO. WHO Global database on child growth and malnutrition. 1997. Geneva: WHO.20. Christie L, Hine RJ, Parker JG, Burks W. Food allergies in children affect nutrient intake and growth. J Am Diet Assoc. 2002. 102:1648–1651.21. Grimshaw KE. Dietary management of food allergy in children. Proc Nutr Soc. 2006. 65:412–417.22. Ukabam SO, Mann RJ, Cooper BT. Small intestinal permeability to sugars in patients with atopic eczema. Br J Dermatol. 1984. 110:649–652.23. Eggesbø M, Botten G, Stigum H. Restricted diets in children with reactions to milk and egg perceived by their parents. J Pediatr. 2001. 139:583–587.24. Agostoni C, Grandi F, Scaglioni S, Gianni ML, Torcoletti M, Radaelli G, Fiocchi A, Riva E. Growth pattern of breastfed and nonbreastfed infants with atopic dermatitis in the first year of life. Pediatrics. 2000. 106:E73.25. Kim JH, Lee HC, Jang JH, Ahn KM, Han YS, Lee SI. Risk factors influencing growth in children with atopic dermatitis. Pediatr Allergy Respir Dis. 2008. 18:339–348.26. Sampson HA. Update on food allergy. J Allergy Clin Immunol. 2004. 113:805–819.27. Han YS, Chung SJ, Cho YY, Choi HM, Ahn KM, Lee SI. Analysis of the rate of sensitization to food allergen in children with atopic dermatitis. Korean J Community Nutr. 2004. 9:90–97.28. Cho GR, Kim MJ, Kim JE, Jung JA. A comparison of the sensitization rate to the cow's milk, egg white and soybean in atopic dermatitis at a single institution in 2002 and 2007. Pediatr Allergy Respir Dis. 2008. 18:283–291.29. Na HY, Song YH, Kim BJ, Yu JH, Hong SJ, Lee SY. Allergen sensitization of severe atopic dermatitis in children under 2 years. Pediatr Allergy Respir Dis. 2009. 19:146–154.30. Gartner LM, Morton J, Lawrence RA, Naylor AJ, O'Hare D, Schanler RJ, Eidelman AI. Breastfeeding and the use of human milk. Pediatrics. 2005. 115:496–506.31. Sampson HA. Role of immediate hypersensitivity in the pathogenesis of atopic dermatitis. Allergy. 1989. 44:Suppl 9. 52–58.32. Weller PF. Eosinophilia. J Allergy Clin Immunol. 1984. 73:1–14.33. Butte N, Cobb K, Dwyer J, Graney L, Heird W, Rickard K. The start healthy feeding guidelines for infants and toddlers. J Am Diet Assoc. 2004. 104:442–454.34. Greer FR, Sicherer SH, Burks AW. Effects of early nutritional interventions on the development of atopic disease in infants and children: the role of maternal dietary restriction, breastfeeding, timing of introduction of complementary foods, and hydrolyzed formulas. Pediatrics. 2008. 121:183–191.35. Luccioli S, Ross M, Labiner-Wolfe J, Fein SB. Maternally reported food allergies and other food-related health problems in infants: characteristics and associated factors. Pediatrics. 2008. 122:Suppl 2. S105–S112.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relationship between Allergen Sensitization and Frequency of Asthma in Preschool Atopic Dermatitis Children
- Food allergy
- Food and house dust mite allergens in children with atopic dermatitis
- Effect of Egg White Elimination Diet on Clinical Progress and Specific IgE Levels in Egg White Sensitized Children with Atopic Dermatitis
- Positive conversion of specific IgE against house dust mite in children with atopic dermatitis under 24 months of age
