Allergy Asthma Immunol Res.
2014 Jul;6(4):304-309. 10.4168/aair.2014.6.4.304.
The Utility of Serum Tryptase in the Diagnosis of Food-Induced Anaphylaxis
- Affiliations
-
- 1Department of Pediatrics, School of Medicine, Institute of Medicine, Suranaree University of Technology, Nakhonratchasima, Thailand.
- 2Division of Allergy and Immunology, Department of Pediatrics, Faculty of Medicine Siriraj Hospital Mahidol University, Bangkok, Thailand. siojr@mahidol.ac.th
- 3Institute of Molecular Biosciences, Mahidol University, Nakhonpathom, Thailand.
- KMID: 2260210
- DOI: http://doi.org/10.4168/aair.2014.6.4.304
Abstract
- PURPOSE
This study investigates the utility of serum tryptase for the confirmation of shrimp-induced anaphylaxis.
METHODS
Patients with a history of shrimp allergy and positive skin prick tests (SPT) to commercial shrimp extract were recruited for shrimp challenges. Serum total tryptase was obtained at baseline and 60 min (peak) after the onset of symptoms.
RESULTS
Thirty-nine patients were challenged. There were 12 patients with anaphylaxis, 20 with mild reactions and 7 without symptoms (control group). Characteristic features and baseline tryptase were not different among the 3 groups. The peak tryptase levels were higher than the baseline in anaphylaxis and mild reaction groups (P<0.05). The delta-tryptase (peak minus baseline) and the tryptase ratio (peak divided by baseline) in the anaphylaxis group were higher than the mild reaction and control groups (P<0.01). The optimum cut-off for peak tryptase to confirm anaphylaxis was 2.99 microg/L with 50% sensitivity, 85% specificity, 3.33 positive likelihood ratio (LR) and 0.59 negative LR. The manufacturer's cut-off for peak tryptase was >11.4 microg/L with 17% sensitivity, 100% specificity, infinity positive LR and 0.83 negative LR. The best cut-off for delta-tryptase was > or =0.8 microg/L with 83% sensitivity, 93% specificity, 11.86 positive LR and 0.18 negative LR. The best cut-off for tryptase ratio was > or =1.5 with 92% sensitivity, 96% specificity, 23 positive LR and 0.08 negative LR.
CONCLUSIONS
The peak tryptase level should be compared with the baseline value to confirm anaphylaxis. The tryptase ratio provide the best sensitivity, specificity, positive and negative LR than a single peak serum tryptase for the confirmation of shrimp-induced anaphylaxis.
Keyword
Figure
-

Fig. 1 The change in the total tryptase in control, mild reaction and anaphylaxis groups during shrimp challenges. Baseline and peak tryptase values are designated by closed squares and closed triangulars, respectively. Horizontal bars indicate medians. NS: not significant.
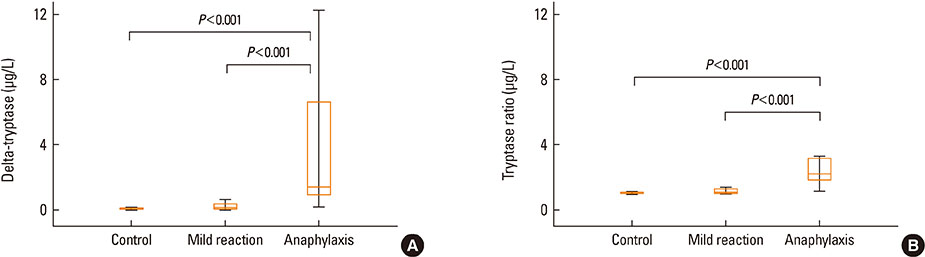
Fig. 2 (A) Box plot of the delta-tryptase values (peak minus baseline tryptase) in control, mild reaction and anaphylaxis groups. (B) The box plot of tryptase ratio values (peak divided by baseline tryptase) in the control, mild reaction and anaphylaxis groups.

Fig. 3 Receiver-operator characteristics (ROC) curve analysis of peak serum tryptase, delta-tryptase and tryptase ratio for the diagnosis of anaphylaxis.
Reference
-
1. Sampson HA, Muñoz-Furlong A, Campbell RL, Adkinson NF Jr, Bock SA, Branum A, Brown SG, Camargo CA Jr, Cydulka R, Galli SJ, Gidudu J, Gruchalla RS, Harlor AD Jr, Hepner DL, Lewis LM, Lieberman PL, Metcalfe DD, O'Connor R, Muraro A, Rudman A, Schmitt C, Scherrer D, Simons FE, Thomas S, Wood JP, Decker WW. Second symposium on the definition and management of anaphylaxis: summary report--Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol. 2006; 117:391–397.2. Lieberman P, Camargo CA Jr, Bohlke K, Jick H, Miller RL, Sheikh A, Simons FE. Epidemiology of anaphylaxis: findings of the American College of Allergy, Asthma and Immunology Epidemiology of Anaphylaxis Working Group. Ann Allergy Asthma Immunol. 2006; 97:596–602.3. Koplin JJ, Martin PE, Allen KJ. An update on epidemiology of anaphylaxis in children and adults. Curr Opin Allergy Clin Immunol. 2011; 11:492–496.4. Lin RY, Anderson AS, Shah SN, Nurruzzaman F. Increasing anaphylaxis hospitalizations in the first 2 decades of life: New York State, 1990-2006. Ann Allergy Asthma Immunol. 2008; 101:387–393.5. Poulos LM, Waters AM, Correll PK, Loblay RH, Marks GB. Trends in hospitalizations for anaphylaxis, angioedema, and urticaria in Australia, 1993-1994 to 2004-2005. J Allergy Clin Immunol. 2007; 120:878–884.6. Jirapongsananuruk O, Bunsawansong W, Piyaphanee N, Visitsunthorn N, Thongngarm T, Vichyanond P. Features of patients with anaphylaxis admitted to a university hospital. Ann Allergy Asthma Immunol. 2007; 98:157–162.7. Simons FE, Frew AJ, Ansotegui IJ, Bochner BS, Golden DB, Finkelman FD, Leung DY, Lotvall J, Marone G, Metcalfe DD, Müller U, Rosenwasser LJ, Sampson HA, Schwartz LB, van Hage M, Walls AF. Risk assessment in anaphylaxis: current and future approaches. J Allergy Clin Immunol. 2007; 120:S2–S24.8. Sampson HA, Mendelson L, Rosen JP. Fatal and near-fatal anaphylactic reactions to food in children and adolescents. N Engl J Med. 1992; 327:380–384.9. Beyer K, Eckermann O, Hompes S, Grabenhenrich L, Worm M. Anaphylaxis in an emergency setting - elicitors, therapy and incidence of severe allergic reactions. Allergy. 2012; 67:1451–1456.10. Lemon-Mulé H, Nowak-Wegrzyn A, Berin C, Knight AK. Pathophysiology of food-induced anaphylaxis. Curr Allergy Asthma Rep. 2008; 8:201–208.11. Brown SG, Blackman KE, Heddle RJ. Can serum mast cell tryptase help diagnose anaphylaxis? Emerg Med Australas. 2004; 16:120–124.12. Shanmugam G, Schwartz LB, Khan DA. Prolonged elevation of serum tryptase in idiopathic anaphylaxis. J Allergy Clin Immunol. 2006; 117:950–951.13. Jirapongsananuruk O, Sripramong C, Pacharn P, Udompunturak S, Chinratanapisit S, Piboonpocanun S, Visitsunthorn N, Vichyanond P. Specific allergy to Penaeus monodon (seawater shrimp) or Macrobrachium rosenbergii (freshwater shrimp) in shrimp-allergic children. Clin Exp Allergy. 2008; 38:1038–1047.14. Thermo Fisher Scientific Inc (SE). ImmunoCAP tryptase. Directions for use [Internet]. Uppsala: Thermo Fisher Scientific Inc.;2012. cited 2013 Jan 12. Available from: http://www.phadia.com/da/Products/Allergy-testing-products/ImmunoCAP-Assays/ImmunoCAP-Tryptase/.15. Brown SG. Clinical features and severity grading of anaphylaxis. J Allergy Clin Immunol. 2004; 114:371–376.16. Vander Leek TK, Liu AH, Stefanski K, Blacker B, Bock SA. The natural history of peanut allergy in young children and its association with serum peanut-specific IgE. J Pediatr. 2000; 137:749–755.17. Pumphrey R. Anaphylaxis: can we tell who is at risk of a fatal reaction? Curr Opin Allergy Clin Immunol. 2004; 4:285–290.18. Braganza SC, Acworth JP, McKinnon DR, Peake JE, Brown AF. Paediatric emergency department anaphylaxis: different patterns from adults. Arch Dis Child. 2006; 91:159–163.19. Brown SGA, Stone SF. Laboratory diagnosis of acute anaphylaxis. Clin Exp Allergy. 2011; 41:1660–1662.20. Stone SF, Cotterell C, Isbister GK, Holdgate A, Brown SG. Emergency Department Anaphylaxis Investigators. Elevated serum cytokines during human anaphylaxis: Identification of potential mediators of acute allergic reactions. J Allergy Clin Immunol. 2009; 124:786–792.e4.21. Yunginger JW, Squillace DL, Jones RT, Helm RM. Fatal anaphylactic reactions induced by peanuts. Allergy Proc. 1989; 10:249–253.22. Sala-Cunill A, Cardona V, Labrador-Horrillo M, Luengo O, Esteso O, Garriga T, Vicario M, Guilarte M. Usefulness and limitations of sequential serum tryptase for the diagnosis of anaphylaxis in 102 patients. Int Arch Allergy Immunol. 2013; 160:192–199.23. Schwartz LB, Irani AM, Roller K, Castells MC, Schechter NM. Quantitation of histamine, tryptase, and chymase in dispersed human T and TC mast cells. J Immunol. 1987; 138:2611–2615.24. Caughey GH. Tryptase genetics and anaphylaxis. J Allergy Clin Immunol. 2006; 117:1411–1414.25. Enrique E, García-Ortega P, Sotorra O, Gaig P, Richart C. Usefulness of UniCAP-Tryptase fluoroimmunoassay in the diagnosis of anaphylaxis. Allergy. 1999; 54:602–606.26. Borer-Reinhold M, Haeberli G, Bitzenhofer M, Jandus P, Hausmann O, Fricker M, Helbling A, Müller U. An increase in serum tryptase even below 11.4 ng/mL may indicate a mast cell-mediated hypersensitivity reaction: a prospective study in Hymenoptera venom allergic patients. Clin Exp Allergy. 2011; 41:1777–1783.27. Ordoqui E, Zubeldia JM, Aranzábal A, Rubio M, Herrero T, Tornero P, Rodriguez VM, Prieto A, Baeza ML. Serum tryptase levels in adverse drug reactions. Allergy. 1997; 52:1102–1105.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Causes and Diagnostic Usefulness of Tryptase Measurements for Anaphylaxis in a Korean Tertiary Care General Hospital
- Elevated level of serum tryptase in a patient with exercise-inuced anaphylaxis
- Recent update on the management of anaphylaxis
- Usefulness of Serum Mast Cell Tryptase Analysis in Postmortem Diagnosis of Anaphylactic Shock
- Food allergies and food-induced anaphylaxis: role of cofactors
