Death due to Cardiac Metastasis after Treatment of Oral Squamous Cell Carcinoma: An Autopsy Case
- Affiliations
-
- 1Division of Forensic Medicine, National Forensic Service, Seoul, Korea. giifpap@korea.kr
- KMID: 2250328
- DOI: http://doi.org/10.7580/KoreanJLegMed.2012.36.1.115
Abstract
- A 60-year-old man presented with electrocardiographic abnormalities after treatment for oral squamous cell carcinoma with surgical resection and radiation therapy 7 months ago. The patient died within 2 h without response to CPR after sudden arrest. Electrocardiographic changes 9 h before death included low QRS voltage and sinus tachycardia. Autopsy revealed cardiac metastasis with chronic active fibrinoid pericarditis accompanied by tumor cell infiltration. Although the frequency of cardiac metastasis in patients with oral cancer is reportedly low, clinicians should be aware that cardiac metastasis may exist if there are electrocardiographic changes in patients receiving follow-up care for primary malignancy. We report a rare medicolegal case of cardiac metastasis-related sudden death.
Keyword
MeSH Terms
Figure
-
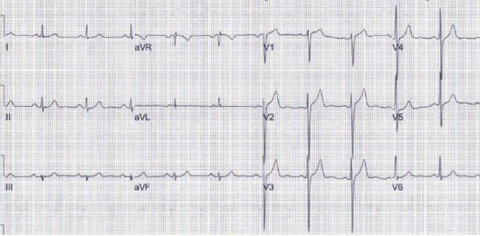
Fig. 1 The deceased's ECG at the time of diagnosis primary oral squamous cell carcinoma showed normal sinus rhythm.
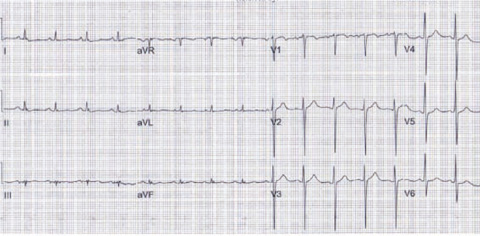
Fig. 2 After treatment of primary oral cancer for 7 months, the deceased presented ECG abnormalities as sinus tachycardia and low voltage QRSs.

Fig. 3 The pericardium typically has the feature of chronic constrictive pericarditis with hemorrhage and fibrinoid exudation (a and b). The metastatic tumor mass bulges in and out the right atrial wall (c and d).

Fig. 4 The metastatic tumor mass with a central necrosis is formed along the right atrioventricular groove, encircling the proximal portion of the right coronary artery.

Fig. 5 Histologically, the tumor mass is consistent with well differentiated squamous cell carcinoma (A). Tumor cells infiltrate deep to the endothelium of the right coronary artery, making a focal thrombosis (B). Tumor emboli are found in the anterior right atrial branch of the right coronary artery and a few small vessels near the nodal tissues (C). The pericardium is infiltrated with squamous cell carcinoma cells and accompanies fibronoid exudation and inflammation (D).
Reference
-
1. Oliveira SM, Goncalves A, Cruz C, et al. Cardiac metastasis from epidermoid esophageal cancer mimicking anterior myocardial infactrion. Rev Port Cardiol. 2011. doi:10.1016/j.repc.2011.12.011.2. Karwinski B, Svendsen E. Trends in cardiac metastasis. APMIS. 1989. 97:1018–1024.3. Abraham KP, Reddy V, Gattuso P. Neoplasms metastatic to the heart: review of 3314 consecutive autopsies. Am J Cardiovasc Pathol. 1990. 3:195–198.4. Al-Mamgani A, Baartman L, Baaijens M, de Pree I, Incrocci L, Levendag PC. Cardiac metastases. Int J Clin Oncol. 2008. 13:369–372.5. Ito T, Ishikawa N, Negishi T, Ohno K. Cardiac metastasis of tongue cancer may cause sudden death. Auris Nasus Larynx. 2008. 35:423–425.6. Astorri E, Bonetti A, Fiorina P. ECG mimicking acute myocardial infarction during heart involvement by lung neoplasm. Int J Cardiol. 2000. 74:225–226.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Synchronous thyroid carcinoma and squamous cell carcinoma: A case report
- Clinicopathologic parameters in predicting cervical nodal metastasis in early squamous cell carcinoma of the oral cavity
- A Case of Squamous Cell Carcinoma of Cervical Esophagus with Metastasis to Thyroid Gland
- A Case of Metastatic Squamous Cell Carcinoma of the Choroid
- Diagnostic problem of squamous papilloma and oral mucosa malignancy