J Gynecol Oncol.
2012 Jul;23(3):201-204. 10.3802/jgo.2012.23.3.201.
Successful term pregnancies after laparoscopic excision of poorly differentiated Sertoli-Leydig cell tumor of the ovary
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Sultan Qaboos University Hospital, Sultan Qaboos University College of Medicine, Muscat, Sultanate of Oman. gowri@squ.edu.om
- 2Department of Surgery, Sultan Qaboos University Hospital, Sultan Qaboos University College of Medicine, Muscat, Sultanate of Oman.
- 3Department of Pathology, Sultan Qaboos University Hospital, Sultan Qaboos University College of Medicine, Muscat, Sultanate of Oman.
- KMID: 2245181
- DOI: http://doi.org/10.3802/jgo.2012.23.3.201
Abstract
- Ovarian Sertoli-Leydig cell tumors are rare sex cord-stromal tumors, accounting for less than 1% of ovarian tumors. Majority of these tumors are benign and unilateral, only 3-5% are bilateral. These patients present with clinical features of virilization due to excessive secretion of testosterone from the tumor, however 50% may have no endocrine symptoms. We report a case of poorly differentiated Sertoli-Leydig cell tumour in a woman diagnosed during routine investigation of infertility. She had two spontaneous successful pregnancies after tumor excision laparoscopically.
Keyword
MeSH Terms
Figure
-
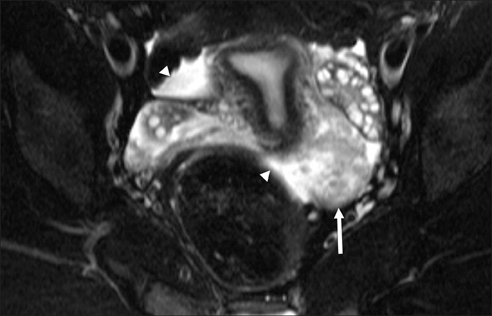
Fig. 1 Axial fat saturated T2 weighted image of pelvis showing uterus and both ovaries identified a heterogeneous solid mass close to the left ovary (arrow) and a small amount of free fluid in the pelvis (arrowheads).
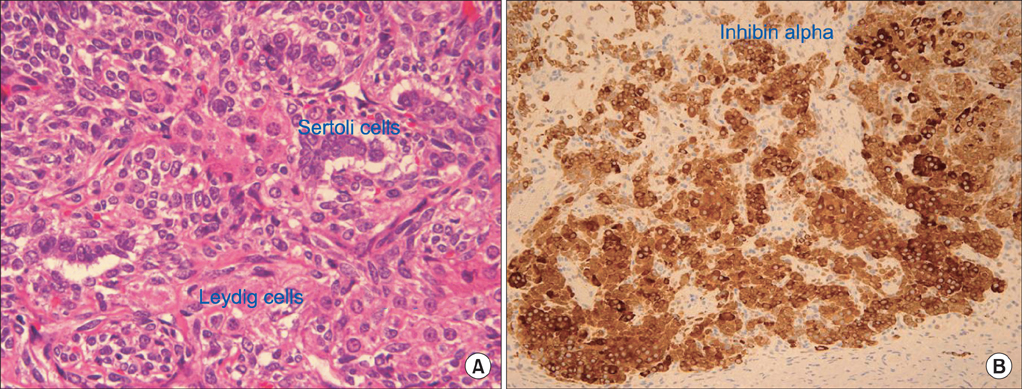
Fig. 2 (A) Sertoli cells surrounded by Leydig cells (H&E, ×60). (B) Immunohistochemistry studies showing strong positive staining for inhibin (×20).
Reference
-
1. Roth LM, Anderson MC. Sertoli Leydig cell tumors: a clinicopathologic study of 34 cases. Cancer. 1981. 48:187–197.2. Oliva E, Alvarez T, Young RH. Sertoli cell tumors of the ovary: a clinicopathologic and immunohistochemical study of 54 cases. Am J Surg Pathol. 2005. 29:143–156.3. Pride GL, Pollock WJ, Norgard MJ. Metastatic Sertoli-Leydig cell tumor of the ovary during pregnancy treated by BV-CAP chemotherapy. Am J Obstet Gynecol. 1982. 143:231–233.4. Young RH, Scully RE. Ovarian Sertoli-Leydig cell tumors: a clinicopathological analysis of 207 cases. Am J Surg Pathol. 1985. 9:543–569.5. Sachdeva P, Arora R, Dubey C, Sukhija A, Daga M, Singh DK. Sertoli-Leydig cell tumor: a rare ovarian neoplasm: case report and review of literature. Gynecol Endocrinol. 2008. 24:230–234.6. Metzinger DS, Webb MJ. Surgical management of Sertoli-Leydig cell tumors of the ovary. CME J Gynecol Oncol. 2002. 7:140–142.7. Zheng W, Senturk BZ, Parkash V. Inhibin immunohistochemical staining: a practical approach for the surgical pathologist in the diagnoses of ovarian sex cord-stromal tumors. Adv Anat Pathol. 2003. 10:27–38.8. Toppari J, Kaipia A, Kaleva M, Laato M, de Kretser DM, Krummen LA, et al. Inhibin gene expression in a large cell calcifying Sertoli cell tumour and serum inhibin and activin levels. APMIS. 1998. 106:101–112.9. Ohashi M, Hasegawa Y, Haji M, Igarashi M, Nawata H. Production of immunoreactive inhibin by a virilizing ovarian tumour (Sertoli-Leydig tumour). Clin Endocrinol (Oxf). 1990. 33:613–618.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Giant Sertoli-Leydig Cell Tumor of the Ovary with Masculinization
- Ovarian serous cystadenoma associated with Sertoli-Leydig cell tumor: a case report
- A Case of Sertoli-Leydig Cell Tumor Combined with Dermoid Cyst
- Two Cases of Sertoli-Leydig Cell Tumor of Ovary
- Sertoli-Leydig Cell Tumor of Hemangiopericytoma Pattern: A case report
