Successful percutaneous management of bronchobiliary fistula after radiofrequency ablation of metastatic cholangiocarcinoma in a patient who has a postoperative stricture of hepaticojejunostomy site
- Affiliations
-
- 1Department of Surgery, Wonkwang University Hospital, Wonkwang University School of Medicine, Iksan, Korea. Knife@wonkwang.ac.kr
- KMID: 2243216
- DOI: http://doi.org/10.14701/kjhbps.2012.16.3.110
Abstract
- Bronchobiliary fistula (BBF) is a rare condition that is defined as an abnormal communication between the biliary system and bronchial tree. Furthermore, a BBF is an extremely rare complication of radiofrequency ablation (RFA). A 54 year-old man with a history of extrahepatic biliary cancer had been suffering with a benign stricture of hepaticojejunostomy site and was treated with RFA for metastatic cholangicarcinoma. In this report, we describe a patient with BBF complicated by an abscess which occurred after RFA. He was treated by placement of external drainage catheter into the liver abscess and percutaneous transhepatic biliary drainage (PTBD) into the right intrahepatic duct. After 6 weeks, a complete obliteration of the BBF was confirmed by a repeated follow-up of computed tomography scan and cholangiography through PTBD.
MeSH Terms
Figure
-

Fig. 1 A computed tomography scan obtained two weeks after radiofrequency ablation shows that the previously ablated area has become hypodense with area formation, which was identified as a liver abscess (arrow).
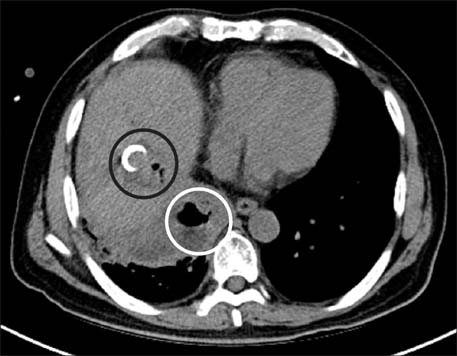
Fig. 2 A follow-up computed tomography shows liver abscess with inserted pigtail catheter in the previous radiofrequency ablated site (black circle) and consolidation with air formation in the adjacent diaphragm, which was diagnosed as a lung abscess (white circle).
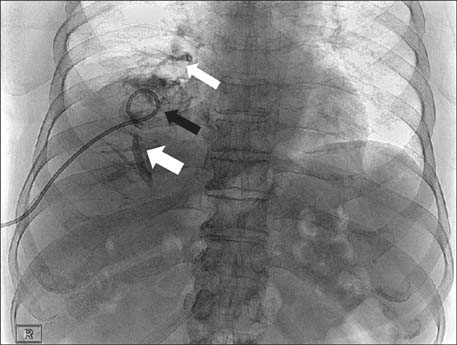
Fig. 3 Contrast material was injected through the percutaneous abscess drainage catheter. This contrast material showed in the abscess cavity in liver (black arrow), bronchial tree (thin white arrow), and biliary tree (wide white arrow), confirming the presence of bronchobiliary fistula.

Fig. 4 Although the amount of sputum decreased after the insertion of the drainage catheter, bilioptysis and coughing continued. We performed percutaneous transhepatic biliary drainage (PTBD) in the dilated right hepatic duct to reduce the intrahepatic biliary tree pressure which was increased due to the hepaticojejunostomy site stricture.

Fig. 5 One month later, the follow-up coronary computed tomography image shows improvement of liver abscess and no consolidation of lower lung field.

Fig. 6 After the percurtaneous drainage catheter was removed, contrast material was injected through PTBD catheter. Cholangiography shows no communication between the bronchial system and biliary tree.
Reference
-
1. Peacock TB. Case in which hydatids were expectorated and one of suppuration of hydatid cyst of the liver communicating with the lungs. Edinburgh Med J. 1850. 74:33–46.2. Liao GQ, Wang H, Zhu GY, et al. Management of acquired bronchobiliary fistula: A systematic literature review of 68 cases published in 30 years. World J Gastroenterol. 2011. 17:3842–3849.3. Cropper LD Jr, Gold RE, Roberts LK. Bronchobiliary fistula: management with percutaneous catheter drainage of a subphrenic abscess. J Trauma. 1982. 22:68–70.4. Sutherland RD, Reynolds J, Sugg WL. Bile ptyalism associated with chest trauma and sickle cell crisis simulating bronchobiliary fistula. Ann Thorac Surg. 1972. 13:537–542.5. Moumen M, el Fares F. Bilio-bronchial fistula of hydatid origin. Apropos of 8 cases. J Chir (Paris). 1991. 128:188–192.6. Ong M, Moozar K, Cohen LB. Octreotide in bronchobiliary fistula management. Ann Thorac Surg. 2004. 78:1512–1513.7. Gugenheim J, Ciardullo M, Traynor O, et al. Bronchobiliary fistulas in adults. Ann Surg. 1988. 207:90–94.8. Kim JH, Kim MD, Lee YK, et al. Bronchobiliary fistula treated with histoacryl embolization under bronchoscopic guidance: A case report. Respir Med CME. 2008. 1:164–168.9. Goldman SY, Greben CR, Setton A, et al. Bronchobiliary fistula successfully treated with n-butyl cyanoacrylate via a bronchial approach. J Vasc Interv Radiol. 2007. 18:151–155.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Management of a Bronchobiliary Fistula after Radiofrequency Ablation in a Patient with Hepatocellular Carcinoma
- Surgical Treatment of Bronchobiliary Fistula with Pulmonary Resection and Omentopexy
- Surgical treatment of bronchobiliary fistula due to radiofrequency ablation for recurrent hepatocellular carcinoma
- Successful Management of Atrio-Esophageal Fistula after Cardiac Radiofrequency Catheter Ablation
- A Case of Bronchobiliary Fistula as a Complication of Radiofrequency Ablation
