Korean J Hepatobiliary Pancreat Surg.
2012 Nov;16(4):142-146. 10.14701/kjhbps.2012.16.4.142.
Extent of resection for T2N0 gallbladder carcinoma regarding concurrent extrahepatic bile duct resection
- Affiliations
-
- 1Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. shwang@amc.seoul.kr
- KMID: 2243192
- DOI: http://doi.org/10.14701/kjhbps.2012.16.4.142
Abstract
- BACKGROUNDS/AIMS
Gallbladder carcinoma (GBCa) T2 lesions are considered to be advanced tumors showing diverse features in tumor extent. When this T2 lesion does not involve the cystic duct and there is no evidence of lymph node metastasis, we have to consider what is the most reasonable extent of resection - that is, whether to perform concurrent extra-hepatic bile duct resection (EHBD) resection or not. This study intends to evaluate the adequacy of EHBD resection in patients undergoing resection for T2N0 GBCa.
METHODS
From our institutional database of GBCa, 48 cases of T2N0 GBCa who underwent R0 resection during November 1995 and August 2008 were selected. Patients who underwent prior laparoscopic cholecystectomy were excluded. Their medical records were reviewed retrospectively.
RESULTS
Their mean age was 63.2+/-83.3 years and females were 25. The mean serum CA19-9 level was 37.3+/-89.3 ng/ml. The extents of liver resection were wedge resection (n=36) and segment 4a+5 resection (n=12). Concurrent EHBD resection was performed in 16 (33.3%) patients. No fatal surgical complication occurred. The majority of tumor pathology was adenocarcinoma (n=42), with additional unusual types as papillary (n=3), saromatoid (n=1), signet ring cell (n=1) and adenosquamous (n=1) cancers. The overall survival rate was 87.1% at 1 year, 69.5% at 3 years and 61.7% at 5 years. After exclusion of mortalities not related to cancer, the overall patient survival rate was 89.6% at 1 year, 72.9% at 3 years and 64.7% at 5 years, with 3-year survival rates of 72% in the EHBD resection group and 69.2% in the non-resection group (p=0.661).
CONCLUSIONS
The results of this study indicate that concurrent EHBD resection did not improve patient survival when R0 resection was achieved in patients with T2N0 GBCa. Therefore, routine EHBD resection may not be indicated for T2N0 GBCa unless the tumor is close to the cystic duct.
Keyword
MeSH Terms
Figure
-
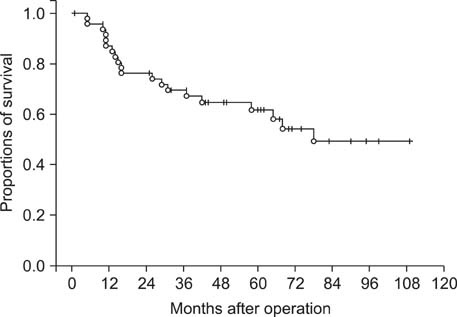
Fig. 1 The overall survival curve of 48 patients with pT2N0 gallbladder carcinoma.

Fig. 2 Comparison of the overall patient survival curves according to the extrahepatic bile duct resection.

Fig. 3 Comparison of the overall patient survival curves according to the extrahepatic bile duct resection, with exclusion of mortalities not related to cancer recurrence.
Reference
-
1. Kohya N, Miyazaki K. Hepatectomy of segment 4a and 5 combined with extra-hepatic bile duct resection for T2 and T3 gallbladder carcinoma. J Surg Oncol. 2008. 97:498–502.2. Nimura Y. Extended surgery in bilio-pancreatic cancer: the Japanese experience. Semin Oncol. 2002. 29:6 Suppl 20. 17–22.3. Tsukada K, Hatakeyama K, Kurosaki I, et al. Outcome of radical surgery for carcinoma of the gallbladder according to the TNM stage. Surgery. 1996. 120:816–821.4. Wakai T, Shirai Y, Yokoyama N, et al. Early gallbladder carcinoma does not warrant radical resection. Br J Surg. 2001. 88:675–678.5. Shimizu Y, Ohtsuka M, Ito H, et al. Should the extrahepatic bile duct be resected for locally advanced gallbladder cancer? Surgery. 2004. 136:1012–1017.6. Shukla PJ, Barreto SG, Shrikhande SV, et al. Simultaneous gallbladder and bile duct cancers: revisiting the pathological possibilities. HPB (Oxford). 2008. 10:48–53.7. Nagata E, Sakai K, Kinoshita H, et al. The relation between carcinoma of the gallbladder and an anomalous connection between the choledochus and the pancreatic duct. Ann Surg. 1985. 202:182–190.8. Funabiki T, Matsubara T, Miyakawa S, et al. Pancreaticobiliary maljunction and carcinogenesis to biliary and pancreatic malignancy. Langenbecks Arch Surg. 2009. 394:159–169.9. Srivastava M, Sharma A, Kapoor VK, et al. Stones from cancerous and benign gallbladders are different: A proton nuclear magnetic resonance spectroscopy study. Hepatol Res. 2008. 38:997–1005.10. Kozuka S, Tsubone M, Hachisuka K. Evolution of carcinoma in the extrahepatic bile ducts. Cancer. 1984. 54:65–72.11. Chijiiwa K. Synchronous carcinoma of the gall-bladder in patients with bile duct carcinoma. Aust N Z J Surg. 1993. 63:690–692.12. Nakamura S, Sakaguchi S, Suzuki S, et al. Aggressive surgery for carcinoma of the gallbladder. Surgery. 1989. 106:467–473.13. Matsumoto Y, Fujii H, Aoyama H, et al. Surgical treatment of primary carcinoma of the gallbladder based on the histologic analysis of 48 surgical specimens. Am J Surg. 1992. 163:239–245.14. Tsukada K, Hatakeyama K, Kurosaki I, et al. Outcome of radical surgery for carcinoma of the gallbladder according to the TNM stage. Surgery. 1996. 120:816–821.15. Sakamoto Y, Kosuge T, Shimada K, et al. Clinical significance of extrahepatic bile duct resection for advanced gallbladder cancer. J Surg Oncol. 2006. 94:298–306.16. Suzuki S, Yokoi Y, Kurachi K, et al. Appraisal of surgical treatment for pT2 gallbladder carcinomas. World J Surg. 2004. 28:160–165.17. Shimada H, Endo I, Togo S, et al. The role of lymph node dissection in the treatment of gallbladder carcinoma. Cancer. 1997. 79:892–899.18. Nagakura S, Shirai Y, Yokoyama N, et al. Clinical significance of lymph node micrometastasis in gallbladder carcinoma. Surgery. 2001. 129:704–713.19. Chijiiwa K, Noshiro H, Nakano K, et al. Role of surgery for gallbladder carcinoma with special reference to lymph node metastasis and stage using western and Japanese classification systems. World J Surg. 2000. 24:1271–1276.20. Chijiiwa K, Nakano K, Ueda J, et al. Surgicaltreatment of patients with T2 gallbladder carcinoma invading the subserosal layer. J Am Coll Surg. 2001. 192:600–607.21. Kokudo N, Makuuchi M, Natori T, et al. Strategies for surgical treatment of gallbladder carcinoma based on information available before resection. Arch Surg. 2003. 138:741–750.22. Pawlik TM, Gleisner AL, Vigano L, et al. Incidence of finding residual disease for incidental gallbladder carcinoma: implications for re-resection. J Gastrointest Surg. 2007. 11:1478–1486.23. Muratore A, Polastri R, Bouzari H, et al. Radical surgery for gallbladder cancer: a worthwhile operation? Eur J Surg Oncol. 2000. 26:160–163.24. Behari A, Sikora SS, Wagholikar GD, et al. Longtermsurvival after extended resections in patients with gallbladder cancer. J Am Coll Surg. 2003. 196:82–88.25. Bartlett DL, Fong Y, Fortner JG, et al. Long-term results after resection for gallbladder cancer. Implications for staging and management. Ann Surg. 1996. 224:639–646.26. Misra S, Chaturvedi A, Misra NC, et al. Carcinoma of the gallbladder. Lancet Oncol. 2003. 4:167–176.27. Reid KM, Ramos-De la Medina A, et al. Diagnosis and surgical management of gallbladder cancer: a review. J Gastrointest Surg. 2007. 11:671–681.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Review of Carcinomas of the Extrahepatic Bile Ducts and Gallbladders
- Should the Extrahepatic Bile Duct be Resected for T2 Gallbladder Cancer?
- Concurrent Yellow-to-white and Black Extrahepatic Bile Duct Stones
- Hilar portal vein wedge resection and patch venoplasty in patients undergoing bile duct resection for hepatobiliary malignancy: A report of two cases
- Extent of Surgical Resection in Gallbladder Cancer
