Wide-Awake Primary Flexor Tendon Repair, Tenolysis, and Tendon Transfer
- Affiliations
-
- 1Department of Hand Surgery, The Hand Surgery Research Center, Affiliated Hospital of Nantong University, Nantong, China. jinbotang@yahoo.com
- KMID: 2234079
- DOI: http://doi.org/10.4055/cios.2015.7.3.275
Abstract
- Tendon surgery is unique because it should ensure tendon gliding after surgery. Tendon surgery now can be performed under local anesthesia without tourniquet, by injecting epinephrine mixed with lidocaine, to achieve vasoconstriction in the area of surgery. This method allows the tendon to move actively during surgery to test tendon function intraoperatively and to ensure the tendon is properly repaired before leaving the operating table. I applied this method to primary flexor tendon repair in zone 1 or 2, tenolysis, and tendon transfer, and found this approach makes tendon surgery easier and more reliable. This article describes the method that I have used for tendon surgery.
Keyword
MeSH Terms
-
Anesthetics, Local/administration & dosage/therapeutic use
Epinephrine/administration & dosage/therapeutic use
Humans
Range of Motion, Articular
Suture Techniques
*Tendon Injuries/rehabilitation/surgery
Tendon Transfer/*methods
Tendons/*surgery
Vasoconstrictor Agents/administration & dosage/therapeutic use
Anesthetics, Local
Epinephrine
Vasoconstrictor Agents
Figure
-

Fig. 1 The pre-mixed anesthetic solution used for injection and the injection needle (25 or 27 gauge).

Fig. 2 Wide-awake local anesthesia for a case with a complete zone 2 flexor tendon cut in the middle finger. (A) The first injection (10-15 mL) was performed in the most proximal part of the likely dissection to block the nerves distally. (B) Fifteen minutes after the first injection, the second injection (2 mL) was performed subcutaneously at the palmar digital crease between both digital nerves. (C) The third injection (2 mL) was performed immediately after the second injection under the skin at the digital crease of the proximal interphalangeal joint between both digital nerves. (D) The final injection (1 mL) was performed immediately after the third injection under the skin at the digital crease of the distal interphalangeal joint between both digital nerves.

Fig. 3 Thirty minutes after the local anesthesia injection, the epinephrine takes effect. The skin of the operative field has turned pale. The wound was exposed through a Bruner incision, and the distal half of the A2 pulley was incised through the volar midline. The proximal end of ruptured tendon was found in a small incision in the distal palm and advanced under the preserved A1 and the proximal part of the A2 pulleys. This flexor digitorum profundus tendon shown was repaired with a 6-strand M-Tang technique.

Fig. 4 Either a M-shaped 6-strand repair with 4-0 looped suture (A) or a 6-strand asymmetric Kessler repair using 4-0 suture (B) is used. A simple running peripheral suture is added later.

Fig. 5 Sufficient core suture purchase (> 7 mm) and slight tension over the repaired segment are two important elements in surgical repair, making the sutured tendon segment slightly tensioned by creating about 10% shortening in the sutured segment. (A, B) The length of core suture purchase and the direction of slight tension (arrows) in the two repair methods.

Fig. 6 After flexor digitorum profundus tendon repair, the patient actively extended and flexed the finger to perform the extension-flexion test. The photo shows active extension of the repaired digit without gapping at the repair site.

Fig. 7 Postoperative motion: full passive digital flexion (A) is done first, followed by partial active motion (B) in the first 3 weeks.
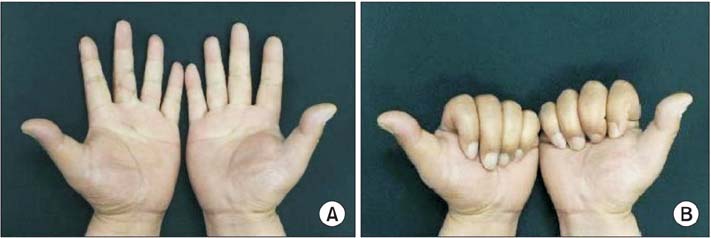
Fig. 8 Follow-up at six months after surgery. (A) Full range of active extension of the left middle finger was achieved without extension deficits of the finger joints. (B) Full range of active flexion.
Cited by 1 articles
-
Wide-Awake Hand surgery
Young Woo Kim
Arch Hand Microsurg. 2021;26(1):1-11. doi: 10.12790/ahm.20.0073.
Reference
-
1. Thomson CJ, Lalonde DH, Denkler KA, Feicht AJ. A critical look at the evidence for and against elective epinephrine use in the finger. Plast Reconstr Surg. 2007; 119(1):260–266.2. Nodwell T, Lalonde D. How long does it take phentolamine to reverse adrenaline-induced vasoconstriction in the finger and hand? A prospective, randomized, blinded study: the Dalhousie project experimental phase. Can J Plast Surg. 2003; 11(4):187–190.3. Lalonde D, Bell M, Benoit P, Sparkes G, Denkler K, Chang P. A multicenter prospective study of 3,110 consecutive cases of elective epinephrine use in the fingers and hand: the Dalhousie Project clinical phase. J Hand Surg Am. 2005; 30(5):1061–1067.4. Fitzcharles-Bowe C, Denkler K, Lalonde D. Finger injection with high-dose (1:1,000) epinephrine: does it cause finger necrosis and should it be treated? Hand (N Y). 2007; 2(1):5–11.5. Mustoe TA, Buck DW 2nd, Lalonde DH. The safe management of anesthesia, sedation, and pain in plastic surgery. Plast Reconstr Surg. 2010; 126(4):165e–176e.6. Lalonde DH. "Hole-in-one" local anesthesia for wide-awake carpal tunnel surgery. Plast Reconstr Surg. 2010; 126(5):1642–1644.7. Tang JB. Clinical outcomes associated with flexor tendon repair. Hand Clin. 2005; 21(2):199–210.8. Tang JB. Release of the A4 pulley to facilitate zone II flexor tendon repair. J Hand Surg Am. 2014; 39(11):2300–2307.9. Tang JB, Zhang Y, Cao Y, Xie RG. Core suture purchase affects strength of tendon repairs. J Hand Surg Am. 2005; 30(6):1262–1266.10. Cao Y, Zhu B, Xie RG, Tang JB. Influence of core suture purchase length on strength of four-strand tendon repairs. J Hand Surg Am. 2006; 31(1):107–112.11. Wu YF, Tang JB. Effects of tension across the tendon repair site on tendon gap and ultimate strength. J Hand Surg Am. 2012; 37(5):906–912.12. Wu YF, Tang JB. Recent developments in flexor tendon repair techniques and factors influencing strength of the tendon repair. J Hand Surg Eur Vol. 2014; 39(1):6–19.13. Higgins A, Lalonde DH, Bell M, McKee D, Lalonde JF. Avoiding flexor tendon repair rupture with intraoperative total active movement examination. Plast Reconstr Surg. 2010; 126(3):941–945.14. Tang JB. Outcomes and evaluation of flexor tendon repair. Hand Clin. 2013; 29(2):251–259.15. Tang JB. Indications, methods, postoperative motion and outcome evaluation of primary flexor tendon repairs in Zone 2. J Hand Surg Eur Vol. 2007; 32(2):118–129.16. Lalonde DH. Wide-awake flexor tendon repair. Plast Reconstr Surg. 2009; 123(2):623–625.17. Lalonde D. Minimally invasive anesthesia in wide awake hand surgery. Hand Clin. 2014; 30(1):1–6.18. Lalonde DH, Martin AL. Wide-awake flexor tendon repair and early tendon mobilization in zones 1 and 2. Hand Clin. 2013; 29(2):207–213.19. Tang JB, Avanessian B. New tendon, nerve, and bone surgical methods impacting the practice of hand surgery. Clin Plast Surg. 2014; 41(3):xix–xxx.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tumescent Local Anesthesia for Hand Surgery: Improved Results, Cost Effectiveness, and Wide-Awake Patient Satisfaction
- Treatment of Massive Defect in Achilles Tendon with Tendon Allograft: A Case Report
- One Stage Flexor Tendon Reconstruction and Early Motion for Old Flexor Tendon Injuries Zone II
- Proximal Flexor Hallucis Longus Tendon Transfer for the Ossification of the Achilles Tendon: A Case Report
- Reconstruction of the Old Flexor Tendon Injury in the Hand
