Successful Treatment with Empirical Erlotinib in a Patient with Respiratory Failure Caused by Extensive Lung Adenocarcinoma
- Affiliations
-
- 1Department of Medicine, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 2Division of Pulmonary and Critical Care Medicine, Department of Medicine, Sungkyunkwan University School of Medicine, Seoul, Korea. sangwonum@skku.edu
- 3Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2227612
- DOI: http://doi.org/10.4266/kjccm.2016.31.1.44
Abstract
- We herein describe a 70-year-old woman who presented with respiratory failure due to extensive lung adenocarcinoma. Despite advanced disease, care in the intensive care unit with ventilator support was performed because she was a newly diagnosed patient and was considered to have the potential to recover after cancer treatment. Because prompt control of the cancer was needed to treat the respiratory failure, empirical treatment with an oral epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor was initiated before confirmation of EGFR-mutant adenocarcinoma, and the patient was successfully treated. Later, EGFR-mutant adenocarcinoma was confirmed.
MeSH Terms
Figure
-

Fig. 1. Chest radiograph (A) and computed tomography scans (B, C) revealed a 3-cm primary mass in the right middle lobe with extensive lung-to-lung metastases forming a confluent mass in both lungs.

Fig. 2. Chest radiograph (A) and computed tomography scans (B, C) revealed a dramatic decrease in the extent of the primary mass and multiple metastatic lesions in both lungs after 3 months of erlotinib treatment.
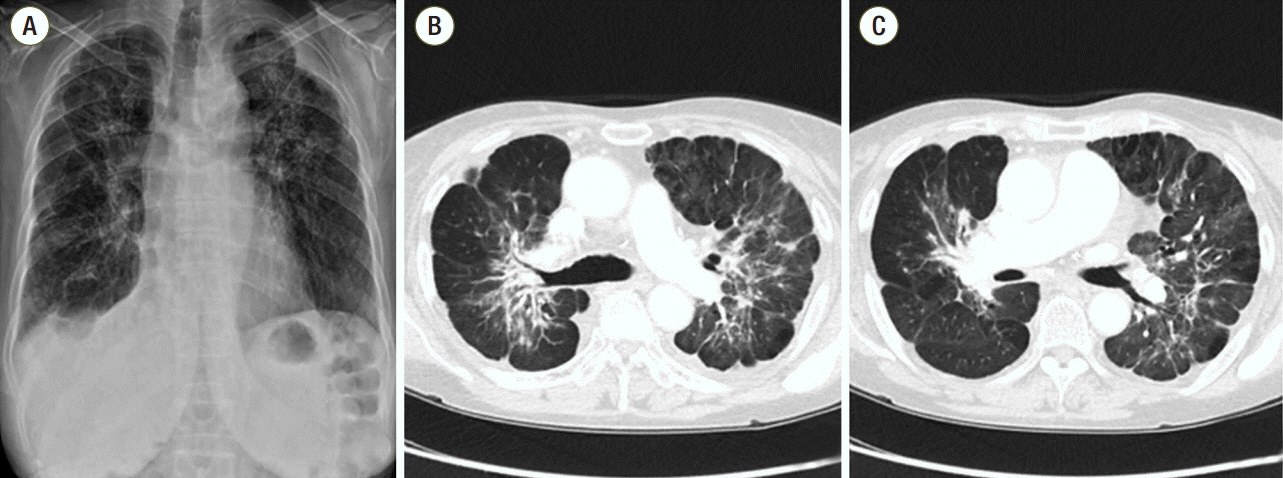
Fig. 3. Chest radiograph (A) and computed tomography scans (B, C) showed an interval decrease in the extent of lung-to-lung metastases in both hemithoraces after 9 months of erlotinib treatment.
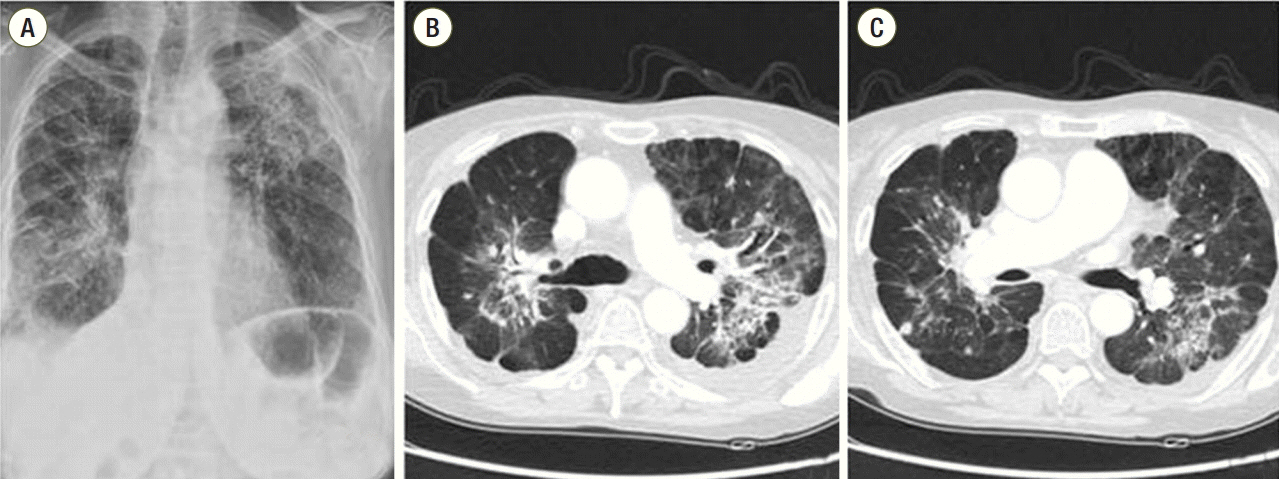
Fig. 4. Chest radiograph (A) and computed tomography scans (B, C) performed after 18 months of treatment showed a slight increase in the extent of the disease.
Reference
-
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015; 65:5–29.
Article2. Adam AK, Soubani AO. Outcome and prognostic factors of lung cancer patients admitted to the medical intensive care unit. Eur Respir J. 2008; 31:47–53.
Article3. Lin YC, Tsai YH, Huang CC, Hsu KH, Wang SW, Tsao TC, et al. Outcome of lung cancer patients with acute respiratory failure requiring mechanical ventilation. Respir Med. 2004; 98:43–51.
Article4. Soubani AO, Ruckdeschel JC. The outcome of medical intensive care for lung cancer patients: the case for optimism. J Thorac Oncol. 2011; 6:633–8.
Article5. Azoulay E, Soares M, Darmon M, Benoit D, Pastores S, Afessa B. Intensive care of the cancer patient: recent achievements and remaining challenges. Ann Intensive Care. 2011; 1:5.
Article6. Cataldo VD, Gibbons DL, Pérez-Soler R, Quintás-Cardama A. Treatment of non-small-cell lung cancer with erlotinib or gefitinib. N Engl J Med. 2011; 364:947–55.
Article7. Kim ES, Hirsh V, Mok T, Socinski MA, Gervais R, Wu YL, et al. Gefitinib versus docetaxel in previously treated non-small-cell lung cancer (INTEREST): a randomised phase III trial. Lancet. 2008; 372:1809–18.
Article8. Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009; 361:947–57.
Article9. Li C, Fang R, Sun Y, Han X, Li F, Gao B, et al. Spectrum of oncogenic driver mutations in lung adenocarcinomas from East Asian never smokers. PLoS One. 2011; 6:e28204.
Article10. Sun Y, Ren Y, Fang Z, Li C, Fang R, Gao B, et al. Lung adenocarcinoma from East Asian never-smokers is a disease largely defined by targetable oncogenic mutant kinases. J Clin Oncol. 2010; 28:4616–20.
Article11. Kim S, Lee J, Hong ME, Do IG, Kang SY, Ha SY, et al. High-throughput sequencing and copy number variation detection using formalin fixed embedded tissue in metastatic gastric cancer. PLoS One. 2014; 9:e111693.
Article12. Darmon M, Thiery G, Ciroldi M, de Miranda S, Galicier L, Raffoux E, et al. Intensive care in patients with newly diagnosed malignancies and a need for cancer chemotherapy. Crit Care Med. 2005; 33:2488–93.
Article13. Bosch-Barrera J, Sais E, Lorencio C, Porta R, Izquierdo A, Menéndez JA, et al. Successful empirical erlotinib treatment of a mechanically ventilated patient newly diagnosed with metastatic lung adenocarcinoma. Lung Cancer. 2014; 86:102–4.
Article14. Ahn HK, Jeon K, Yoo H, Han B, Lee SJ, Park H, et al. Successful treatment with crizotinib in mechanically ventilated patients with ALK positive non-small-cell lung cancer. J Thorac Oncol. 2013; 8:250–3.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful Rechallenge with Gefitinib for an Initial Erlotinib-Responder with Advanced Lung Adenocarcinoma
- Erlotinib-Related Spontaneous Pneumothorax in Patient with Primary Lung Cancer
- Sequential Responses of Adenocarcinoma of the Lung to Erlotinib after Gefitinib in Never Smoker Korean Woman
- Recurrent Erlotinib-Induced Interstitial Lung Disease on Non-Small Cell Lung Cancer
- Comparison of the therapeutic outcome between gefitinib and erlotinib in female patients with non-small-cell lung cancer
