Characteristics of Transplant Coronary Artery Disease after Heart Transplantation in Koreans: A Serial Intravascular UltraSound Analysis
- Affiliations
-
- 1Department of Medicine, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. jjkim@amc.seoul.kr
- KMID: 2227087
- DOI: http://doi.org/10.4070/kcj.2007.37.1.9
Abstract
-
BACKGROUND AND OBJECTIVES: Coronary artery disease (CAD) in a transplanted heart has been a major cause of morbidity and mortality for the transplantation patients who survive more than 1 year. The incidence and characteristic pattern of coronary artery disease after heart transplantation in Koreans are not known. The aim of this study is to determine the incidence and characteristics of significant CAD and the coronary arterial remodeling pattern after heart transplantation by using intravascular ultrasound (IVUS).
SUBJECTS AND METHODS
We evaluated a total of 101 consecutive patients who had been examined via serial (over one year interval) IVUS and coronary angiogram. The patients were divided into two groups according to the period of the serial IVUS follow-up. The post-transplant early period (EP) group (n=58) was defined when IVUS was performed within the first month and at one year after heart transplantation, and the post-transplant late period (LP) group (n=43) was defined when IVUS was performed after one year and subsequently over another one year interval.
RESULTS
The CAD-free survival rates, as assessed by coronary angiogram, were 99% at 5 years, 89% at 7 years and 71% at 9 years. In the EP group, 17 patients (29%) had donor lesions and 8 patients (14%) had de novo lesions. For the donor lesions, the diffuse and concentric lesions were 12%, respectively, and the remodeling index was 2.3+/-6.5, which represents a positive remodeling pattern. For the de novo lesion, the diffuse lesions were 25%, the concentric lesions were 13% and the remodeling index was -2.5+/-4.9, which represent a negative remodeling pattern.
CONCLUSIONS
The incidence of significant CAD with diffuse and concentric lesions after heart transplantation was low in Koreans. The coronary arterial remodeling pattern was negative in the early period, and then it became positive during the late period.
MeSH Terms
Figure
-

Fig. 1 Study design. Patients were subgrouped into an EP group and an LP group. Patients in the EP group were analyzed by IVUS within 1 month after transplantation and then 1 year later. Patients in the LP group were analyzed by IVUS 1 and 3 years after transplantation. HTPL: heart transplantation, EP: post-transplant early period, LP: post-transplant late period, IVUS: intravascular ultrasound.
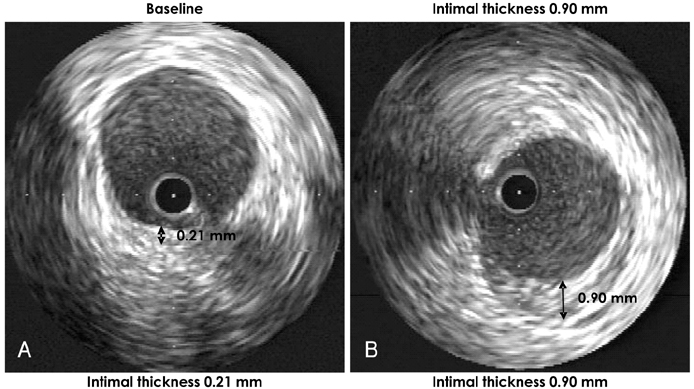
Fig. 2 Intravascular ultrasound (IVUS) images showing the intimal thickness at baseline (A) and after intinal thickness 0.90 mm (B) in one patient, demonstrating de novo lesion. HTPL: heart transplantation, EP: post-transplant early period, LP: post-transplant late period.
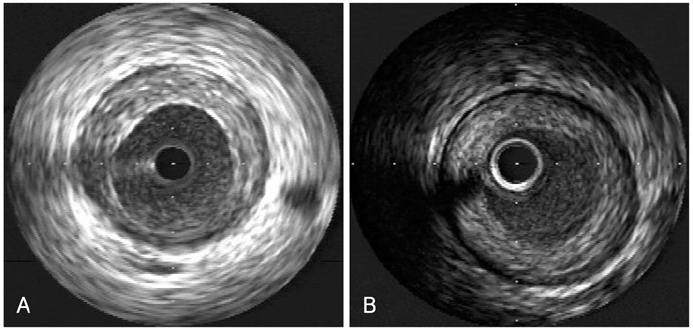
Fig. 3 Intravascular ultrasound (IVUS) showing a coronary arterial eccentric intimal plaque (A) and a concentric intimal plaque (B).

Fig. 4 Calculating the remodeling index (RI). RI was calculated as the change in vessel area/change in the intimal area. An RI ≥1.0 indicates positive remodeling and an RI ≤0 indicates negative remodeling.
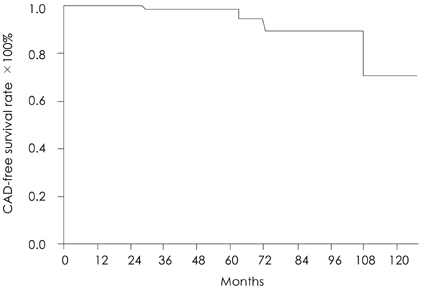
Fig. 5 Angiographical transplant coronary artery disease (CAD) free survival rate. The angiographically significant coronary artery disease-free survival rate was 99% at 5 year, 89% at 7 year and 71% at 9 year.
Reference
-
1. Bieber CP, Hunt SA, Schwinn DA, et al. Complications in long-term survivors of cardiac transplantation. Transplant Proc. 1981. 13:207–211.2. St Goar FG, Pinto FJ, Alderman EL, et al. Intracoronary ultrasound in cardiac transplant recipients: in vivo evidence of 'angiographically silent' intimal thickening. Circulation. 1992. 85:979–987.3. American College of Cardiology. American College of Cardiology Clinical Expert Consensus Document on Standards for Acquisition, Measurement and Reporting of Intravascular Ultrasound Studies: a report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents developed in collaboratoration with the European Society of Cardiology endorsed by the Society of Cardiac Angiography and Interventions. Eur J Echocardiogr. 2001. 2:299–313.4. Lim TT, Liang DH, Botas J, Schroeder JS, Oesterle SN, Yeung AC. Role of compensatory enlargement and shrinkage in transplant coronary artery disease. Circulation. 1997. 95:855–859.5. Hur SH. Lesion characteristics in patients with acute coronary syndrome: a comparison with lesion in patients with stable angina by intravascular ultrasound. Korean Circ J. 2004. 34:548–557.6. Tuzcu EM, Kapadia SR, Sachar R, et al. Intravascular ultrasound evidence of angiographically silent progression in coronary atherosclerosis predicts long-term morbidity and mortality after cardiac transplantation. J Am Coll Cardiol. 2005. 45:1538–1542.7. Kapadia SR, Nissen SE, Ziada KM, et al. Development of transplantation vasculopathy and progression of donor-transmitted atherosclerosis: comparison by serial intravascular ultrasound imaging. Circulation. 1998. 98:2672–2678.8. Rickenbacher PR, Pinto FJ, Lewis NP, et al. Prognostic importance of intimal thickness as measured by intracoronary ultrasound after cardiac transplantation. Circulation. 1995. 92:3445–3452.9. Mehra MR, Ventura HO, Chambers R, et al. Predictive model to assess risk for cardiac allograft vasculopathy: an intravascular ultrasound study. J Am Coll Cardiol. 1995. 26:1537–1544.10. Wiedermann JG, Wasserman HS, Weinberger JZ. Severe intimal thickening by intravascular ultrasonography predicts early death in cardiac transplant recipients. Circulation. 1994. 90:Suppl I. I93.11. Anderson TJ, Meredith IT, Uehata A, et al. Functional significance of intimal thickening as detected by intravascular ultrasound early and late after cardiac transplantation. Circulation. 1993. 88:1093–1100.12. Mainigi SK, Goldberg LR, Sasseen BM, See VY, Wilensky RL. Relative contributions of intimal hyperplasia and vascular remodeling in early cardiac transplant-mediated coronary artery disease. Am J Cardiol. 2003. 91:293–296.13. Glagov S, Weisenberg E, Zarins CK, Stankunavicius R, Kolettis GJ. Compensatory enlargement of human atherosclerotic coronary arteries. N Engl J Med. 1987. 316:1371–1375.14. Gyongyosi M, Yang P, Hassan A, et al. Arterial remodelling of native human coronary arteries in patients with unstable angina pectoris: a prospective intravascular ultrasound study. Heart. 1999. 82:68–74.15. Schwarzacher SP, Uren NG, Ward MR, et al. Determinants of coronary remodeling in transplant coronary disease: a simultaneous intravascular ultrasound and Doppler flow study. Circulation. 2000. 101:1384–1389.16. Schoenhagen P, Ziada KM, Vince DG, Nissen SE, Tuzcu EM. Arterial remodeling and coronary artery disease: the concept of "dilated" versus "obstructive" coronary atherosclerosis. J Am Coll Cardiol. 2001. 38:297–306.17. Hsu RB, Chu SH, Wang SS, et al. Low incidence of transplant coronary disease in Chinese heart recipients. J Am Coll Cardiol. 1999. 33:1573–1577.18. Schmid C, Kerber S, Baba HA, Deng M, Hammel D, Scheld HH. Graft vascular disease after heart transplantation. Eur Heart J. 1997. 18:554–559.19. Park JH, Lee YJ, Kang SJ, et al. Clinical analysis of infections following cardiac transplantation. Korean Circ J. 2001. 31:815–823.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intractable right coronary artery spasm in the early postoperative period after heart transplantation: a case report
- Efficacy of Interavascular Ultrasound in the Palmaz-Schatz Stent Implantation: Clinical Experience of 3 Coronary Artery Disease Patients
- A Case of Coronary Pseudostenosis, Diagnosed by Intravascular Ultrasound
- A Case of Spontaneous Coronary Artery Dissection Healed by Medical Treatment: Serial Findings of Coronary Angiography, Intravascular Ultrasound and Multi-Detector Computed Tomography
- Practical Application of Coronary Imaging Devices in Cardiovascular Intervention
