A Case of Hypertrophic Cardiomyopathy Complicated by Acute Myocardial Infarction and Ventricular Tachycardia: Slow Coronary Artery Flow
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. dgpark@hallym.or.kr
- KMID: 2225793
- DOI: http://doi.org/10.4070/kcj.2008.38.5.291
Abstract
- Many patients with hypertrophic cardiomyopathy experience chest pain, and some of these patients are diagnosed with acute myocardial infarction. Acute myocardial infarction in the setting of hypertrophic cardiomyopathy can occur without coronary atherosclerosis. Although the exact pathophysiologic mechanism of this remains unclear, some pathologic studies have suggested that small vessel coronary artery disease in patients with hypertrophic cardiomyopathy may play a major role in producing myocardial ischemia. Small vessel disease can be suspected when the coronary angiogram shows patent epicardial coronary arteries with slow flow of the angiographic contrast medium. We report here on a case of hypertrophic cardiomyopathy that was complicated with acute myocardial infarction, and this induced catastrophic refractory ventricular tachycardia.
Keyword
MeSH Terms
Figure
-
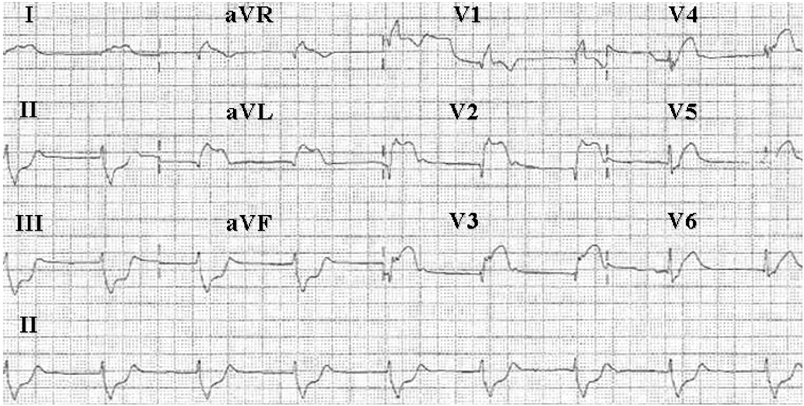
Fig. 1 The electrocardiogram on admission shows ST segment elevation in leads V1-V4 and aVL, and reciprocal ST depression in leads II, III and aVF. aVR: a ventricular right, aVL: a ventricular left, aVF: a ventricular function.

Fig. 2 The left coronary angiography revealed marked slow coronary artery flow, but no significant coronary artery stenosis. The corrected TIMI frame count was 61. TIMI: thrombolysis in myocardial infarction.
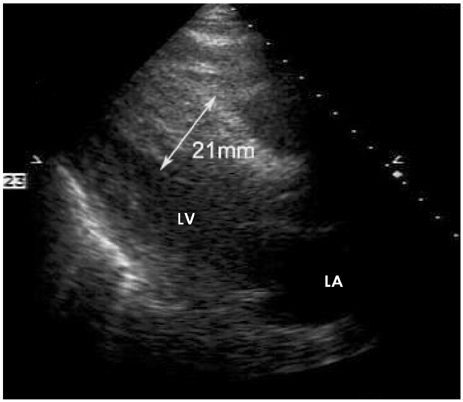
Fig. 3 The echocardiogram demonstrated an interventricular septal wall thickness and a posterior wall thickness of 21 mm and 15 mm, respectively, which was consistent with asymmetric septal hypertrophy. LV: left atrium, LA: left ventricle.

Fig. 4 The electrocardiogram recorded 2 hours after coronary angiography and intraaortic balloon pump insertion shows sustained ventricular tachycardia at 190-200 beats/min.
Cited by 1 articles
-
A Case of Apical Hypertrophic Cardiomyopathy Combined Acute Myocardial Infarction with Multiple Coronary Thrombosis
Kyung-Tae Jung, Soon-Chang Park, Yoo-Jung Choi, Sang Lee, Kyung-Jin Lee, Jung-Hee Kim, Hyun-Soo Yoon
J Cardiovasc Ultrasound. 2008;16(3):96-98. doi: 10.4250/jcu.2008.16.3.96.
Reference
-
1. Zipes DP, Libby P, Bonow RO, Braunwald E. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 2005. 7th ed. Philadelphia: W.B. Saunders Company;1672.2. Gibson CM, Cannon CP, Daley WL, et al. TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation. 1996. 93:879–888.3. Matsuura H. Hypertrophic cardiomyopathy complicated with ventricular aneurysm and myocardial necrosis. J Nucl Med. 1993. 34:2227–2235.4. Lazzeroni E, Rolli A, Aurier E, Botti G. Clinical significance of coronary artery disease in hypertrophic cardiomyopathy. Am J Cardiol. 1992. 70:499–501.5. Richard A, McReynolds RA, Roberts WC. The intramural coronary arteries in hypertrophic cardiomyopathy. Am J Cardiol. 1975. 35:154.6. Maron BJ, Epstein SE, Roberts WC. Hypertrophic cardiomyopathy and transmural myocardial infarction without significant atherosclerosis of the extramural coronary arteries. Am J Cardiol. 1979. 43:1086–1102.7. Maron BJ, Wolfson JK, Epstein SE, Robert WC. Intramural ("small vessel") coronary artery disease in hypertrophic cardiomyopathy. J Am Coll Cardiol. 1986. 8:545–557.8. Aksakal E, Yapici O, Yazici M, Yilmaz O, Sahin M. Apical hypertrophic cardiomyopathy: a case of slow flow in lad and malign ventricular arrhythmia. Int J Cardiovasc Imaging. 2005. 21:185–188.9. Satoshi K, Ichiro I, Takuji K, et al. Intracoronary administration of nicorandil for the treatment of spontaneous microvascular spasm with ST segment elevation. Circ J. 2004. 68:267–269.10. Murakami H, Urabe K, Nishimura M. Inappropriate microvascular constriction produced transient ST-segment elevation in patients with syndrome X. J Am Coll Cardiol. 1998. 32:1287–1294.11. Hahm KB, Lee WK, Cho SY, Park KS, Jang YS, Chung NS. A case of hypertrophic cardiomyopathy with myocardial infarction and normal coronary arteriogram. Korean Circ J. 1986. 16:291–298.12. Dumont CA, Monserrat L, Soler R, et al. Interpretation of electrocardiographic abnormalities in hypertrophic cardiomyopathy with cardiac magnetic resonance. Eur Heart J. 2006. 27:1725–1731.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Apical Hypertrophic Cardiomyopathy Combined Acute Myocardial Infarction with Multiple Coronary Thrombosis
- A Case of Hypertrophic Cardiomyopathy with Myocardial Infarction and Normal Coronary Arteriogram
- A Case of Paroxymal Ventricular Tachycardia Improved due to Electrical Defibrillation was done Repeatedly in Patient with Ce rebral Infarction
- Mid-Ventricular Hypertrophic Obstructive Cardiomyopathy Complicated by an Apical Aneurysm, Presenting as Ventricular Tachycardia
- A Case of Myocardial Bridge in a Patient with Hypertrophic Cardiomyopathy
