Recent Update on Fixed Combinations of Antihypertensive Agents
- Affiliations
-
- 1Division of Cardiology, College of Medicine, Korea University, Seoul, Korea. kuhpark@yahoo.com; parkcg@kumc.or.kr
- KMID: 2225784
- DOI: http://doi.org/10.4070/kcj.2008.38.5.237
Abstract
- The amlodipine/atorvastatin single tablet has been shown to improve patients' achievement of national guideline recommended blood pressure and lipid target levels and exhibits a safety profile consistent with the parent com-pounds. The single tablet formulation has the potential to improve adherence and decrease prescription costs. These potential benefits are associated with important implications because hypertensive patients with additional risk factors represent a large proportion of those at risk for cardiovascular events. Combination low-dose drug treatment increases efficacy and reduces adverse effects. Fixed low-dose combination drug treatment increases efficacy and reduces adverse effects. This combination has greater potency and a similar side effect profile to monotherapy and represents a highly effective approach for attaining goal blood pressure levels using a therapeutic strategy that very effectively lowers blood pressure, is well-tolerated, and minimizes increasing doses of monotherapy-induced metabolic effects.
MeSH Terms
Figure
-
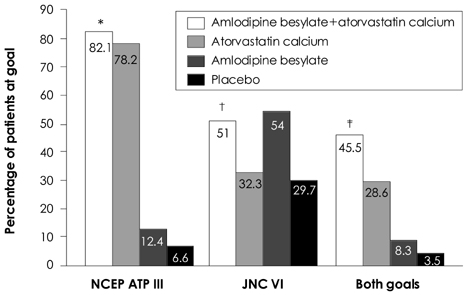
Fig. 1 Efficacy of amlodipine/atorvastatin compared with single-agent therapy or placebo in patients with concomitant hypertension and dyslipidemia. *p=.225 versus atorvastatin; p<.001 versus amlodlpine, †p<.001 versus atorvastatin; p=.520 versus amlodipine, ‡p<.001 versus atorvastatin; p<.001 versus amlodlpine. NCEP ATP III: national cholesterol education program adult treatment panel guideline III, JNC: Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.
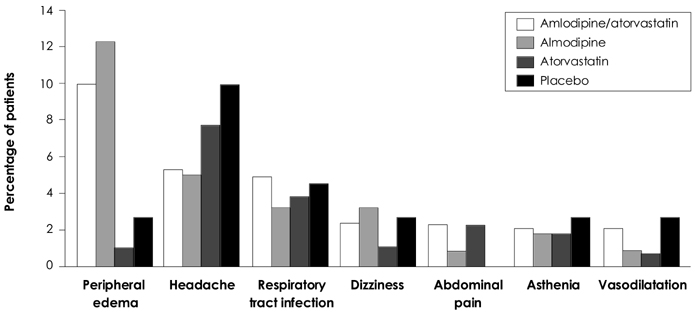
Fig. 2 Tolerability of amlodipine/atorvastatin compared with single-agent therapy or placebo. The graph shows adverse events in patients with co-existing hypertension and dyslipidemia who were randomized to once-daily amlodipine plus atorvastatin (any of eight dose combinations; n=885), amlodipine (5 or 10 mg alone; n=221), atorvastatin (10, 20, 40, or 80 mg alone; n=443), or placebo (n=111) in the double-blind, double-dummy, multicenter RESPOND trial.
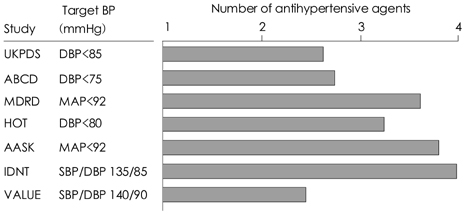
Fig. 3 Two-to-four antihypertensive agents are required to achieve effective BP control to target levels. BP: blood pressure, DBP: diastolic blood pressure, MAP: mean arterial pressure, SBP: systolic blood pressure.
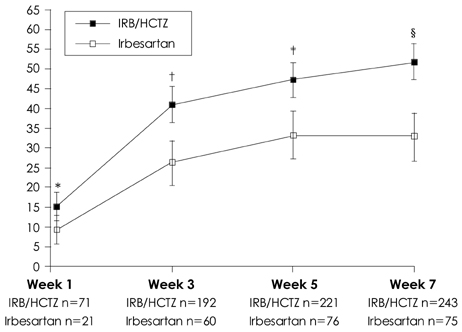
Fig. 4 Comparison of the antihypertensive effects of irbesartan/HCTZ (150/12.5 mg) and valsartan/HCTZ (80/12.5 mg) in hypertensive patients in the COmparative Study of Efficacy of Irbesartan/HCTZ with Valsartan/HCTZ Using Home Blood Pressure Monitoring in the TreAtment of Mild-to-Moderate Hypertension (COSIMA) study.22) *p=0.0317, †p=0.0002, ‡p=0.0005, §p<0.0001. Error bars represent 95% Confidence Intervals. n: number controlled, HCTZ: hydrochlorothiazide.
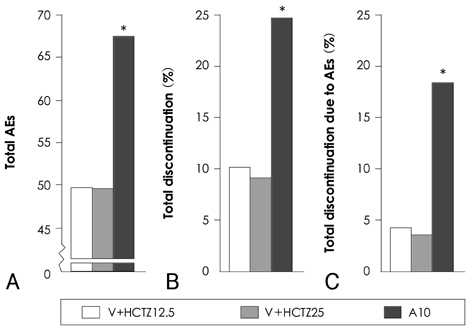
Fig. 5 Rates of (A) total AEs, (B) total discontinuations, and (C) total discontinuations as a result of AEs in the groups that received valsartan (160 mg) plus hydrochlorothiazide (12.5 mg [V+HCTZ12.5]), valsartan (160 mg) plus HCTZ (25 mg [V+HCTZ 2S]), and amlodipine (10 mg [A10]). *p<0.05 vs. combination-therapy groups. HCTZ: hydrochlorothiazide.
Reference
-
1. Kannel WB. Fifty years of Framingham Study contributions to understanding hypertension. J Hum Hypertens. 2000. 14:83–90.2. Health Survey for England. 1998. Available at http://www.archive.official-documents.co.uk/document/doh/survey98/hse-00.htm.3. Asmar R, Vol S, Pannier B, Brisac AM, Tichet J, El Hasnaoui A. High blood pressure and associated cardiovascular risk factors in France. J Hypertens. 2001. 19:1727–1732.4. Chapman RH, Benner JS, Petrilla AA, et al. Predictors of adherence with antihypertensive and lipid-lowering therapy. Arch Intern Med. 2005. 165:1147–1152.5. Agarwal S, McLaughlin T, Joyce A, Schwartz S, Tang S. Synchronizing antihypertensive and lipid-lowering therapies increases patient adherence. J Clin Hypertens. 2006. 8:Suppl A5. A214(P-519). Abstract.6. Dezii CM. A retrospective study of persistence with single-pill combination therapy vs. concurrent two-pill therapy in patients with hypertension. Manag Care. 2000. 9:Suppl. 2–6.7. Safran DG, Neuman P, Schoen C, et al. Prescription drug coverage and seniors: findings from a 2003 national survey. Health Aff (Millwood). 2005. Suppl Web Exclusives:W5-152–W5-66.8. Lee YS, Kim KS. The short-term effect of atorvastatin on flow-mediated vasodilation, pulse wave velocity and carotid intimamedia thickness in patients with moderate cholesterolemia. Korean Circ J. 2008. 38:144–151.9. Blank R, LaSalle J, Reeves R, Maroni J, Tarasenko L, Sun F. Single pill therapy in the treatment of concomitant hypertension and dyslipidemia (the Amlodipine/Atorvastatin Gemini Study). J Clin Hypertens (Greenwich). 2005. 7:264–273.10. Chung M, Calcagni A, Glue P, Bramson C. Effect of food on the bioavailability of amlodipine besylate/atorvastatin calcium combination tablet. J Clin Pharmacol. 2006. 46:1212–1216.11. Chun KJ, Chung NS, Ha JW, et al. Efficacy and safety of atorvastatin in patients with elevated LDL-cholesterolemia. Korean Circ J. 1999. 29:1309–1316.12. Fogari R, Derosa G, Lazzari P, et al. Effect of amlodipine-atorvastatin combination on fibrinolysis in hypertensive hypercholesterolemic patients with insulin resistance. Am J Hypertens. 2004. 17:823–827.13. Preston RA, Sun F, Tarasenko L. Safety and tolerability of coadministered amlodipine and atorvastatin in patients with concomitant hypertension and dyslipidemia in the Respond study. Am J Hypertens. 2005. 18:A92–A93. Abstract.14. Materson BJ, Reda DJ, Cushman WC. Department of veterans Affairs single-drug therapy of hypertension study: revised figures and new data. Am J Hypertens. 1995. 8:189–192.15. Morgan TO, Anderson AI, MacInnis RJ. ACE inhibitors, beta-blockers, calcium blockers, and diuretics for the control of systolic hypertension. Am J Hypertens. 2001. 14:241–247.16. Mancia G, De Backer G, Dominiczak A, et al. 2007 Guidelines for the Management of Arterial Hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2007. 25:1105–1187.17. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003. 289:2560–2572.18. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. N Engl J Med. 2000. 342:145–153.19. Lip GY, Hall JE. Comprehensive Hypertension. 2007. 1st ed. Philadelphia: Mosby Elsevier;1061–1065.20. Bangalore S, Kamalakkannan G, Parkar S, Messerli FH. Fixed-dose combinations improve medication compliance: a meta-analysis. Am J Med. 2007. 120:713–719.21. Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. BMJ. 2003. 326:1427.22. Bobrie G, Delonca J, Moulin C, et al. A home blood pressure monitoring study comparing the antihypertensive efficacy of two angiotensin II receptor antagonist fixed combinations. Am J Hypertens. 2005. 18:1482–1488.23. Flack JM. Maximising antihypertensive effects of angiotensin II receptor blockers with thiazide diuretic combination therapy: focus on irbesartan/hydrochlorothiazide. Int J Clin Pract. 2007. 61:2093–2102.24. Ruilope LM, Malacco E, Khder Y, Kandra A, Bonner G, Heintz D. Efficacy and tolerability of combination therapy with valsartan plus hydrochlorothiazide compared with amlodipine monotherapy in hypertensive patients with other cardiovascular risk factors. Clin Ther. 2005. 27:578–587.25. Andreadis EA, Tsourous GI, Marakomichelakis GE, et al. High-dose monotherapy vs low-dose combination therapy of calcium channel blockers and angiotensin receptor blockers in mild to moderate hypertension. J Hum Hypertens. 2005. 19:491–496.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Principles in the Treatment of Hypertension in the Elderly and New Classes of Antihypertensive Agents
- A study on the withdrawal of the administration of antihypertensive drugs
- Fixed-dose combination therapy for cardiovascular prevention
- Aortic Stiffness in Patients with Deep and Lobar Intracerebral Hemorrhage: Role of Antihypertensive Drugs and Statins
- Antihypertensive drug combinations
