An Overview of Myocardial Bridging With a Focus on Multidetector CT Coronary Angiographic Findings
- Affiliations
-
- 1Department of Radiology, Konkuk University Hospital, Konkuk University School of Medicine, Seoul, Korea. ksm9723@yahoo.co.kr
- KMID: 2225705
- DOI: http://doi.org/10.4070/kcj.2008.38.11.583
Abstract
- Myocardial bridging (MB) is a common anatomical variant rather than a congenital anomaly, and it is usually considered benign. It is generally confined to the mid-portion of the left anterior descending coronary artery. Atherosclerotic plaques are often located in the segment proximal to the bridged segment, although the tunneled segment is typically spared. Conventional coronary angiography is the gold standard for detection, but it is invasive and may not be sensitive enough to detect a thin bridge. The prevalence of MB reported in multidetector CT (MDCT) coronary angiographic series has ranged from 3.5% to 30.5% in patients with chest pain or with suspected or known coronary artery disease. Today, MDCT coronary angiography is an alternative noninvasive imaging tool that allows for easy and accurate evaluation of MB.
MeSH Terms
Figure
-
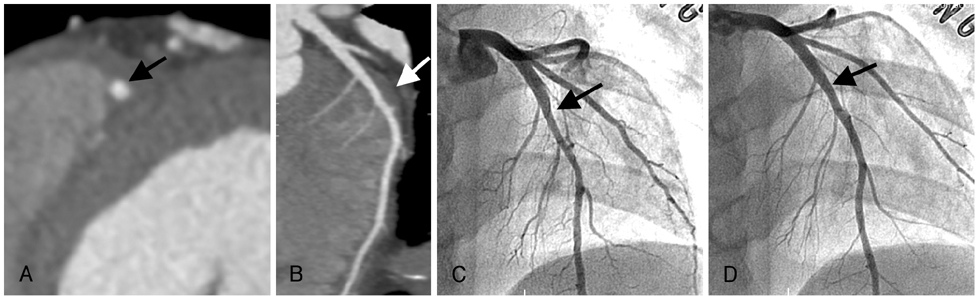
Fig. 1 A 36-year-old man presented with chest pain for 2 weeks. A and B: (A) Short-axis MIP and (B) curved MPR images clearly depict a deep MB segment in the middle segment of the LAD (arrow). C and D: CCA shows that the lumen of the middle segment of the LAD (arrows) is compressed by myocardial contraction in the systolic phase (C), but recovers its normal diameter in the diastolic phase (D). The coronary tree shows no angiographic signs of coronary atherosclerosis. MIP: maximum intensity projection, MPR: multiplanar reconstruction, MB: myocardial bridging, LAD: left anterior descending coronary artery, CCA: conventional coronary angiography.

Fig. 2 Atherosclerotic stenosis proximal to MB in a 67-year-old man presenting with angina. A and B: (A) curved MPR and (B) VR images show a tunneled segment in the mid-LAD (arrows) and calcified plaques in the segments (arrowheads) proximal and distal to the MB, but not within the tunneled segment. C: CCA shows multifocal stenoses in the proximal and distal LAD and the diagonal branches (arrowheads), but no MB was detected in the mid-LAD (arrow). MPR: multiplanar reconstruction, MB: myocardial bridging, LAD: left anterior descending coronary artery, CCA: conventional coronary angiography, VR: volume-rendered.

Fig. 3 Hypertrophic cardiomyopathy in a 66-year-old woman who presented with chest pain on exercise. A and B: (A) short-axis MIP and (B) curved MPR images show the intramyocardial course of the mid-LAD (arrows) and asymmetric wall thickening, mainly in the septum and anterior wall of the left ventricle. MIP: maximum intensity projection, MPR: multiplanar reconstruction, LAD: left anterior descending coronary artery.
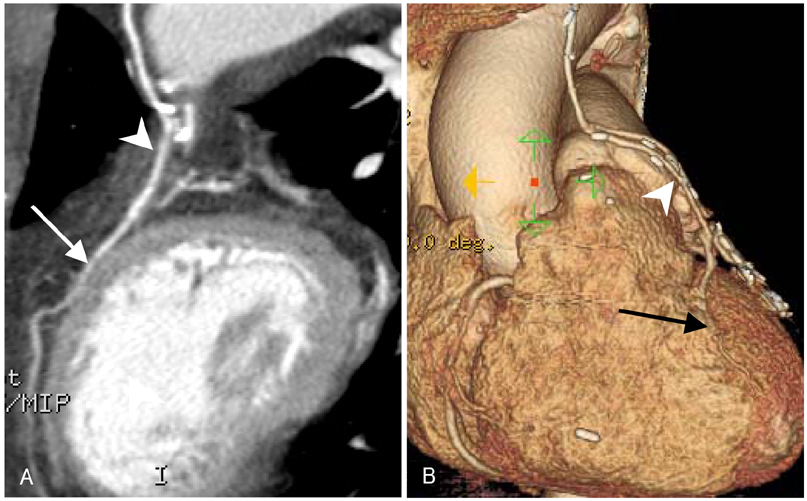
Fig. 4 A 76-year-old woman who underwent MDCT for evaluation of the patency of a coronary artery bypass graft. (A) Curved MPR and (B) VR images show a short segment in the middle part of the LAD (arrows) encased by myocardium, along with a patent left internal mammary artery-LAD graft (arrowheads) proximal to the MB segment. MDCT: multidetector CT, MPR: multiplanar reconstruction, MB: myocardial bridging, LAD: left anterior descending coronary artery, VR: volume-rendered.
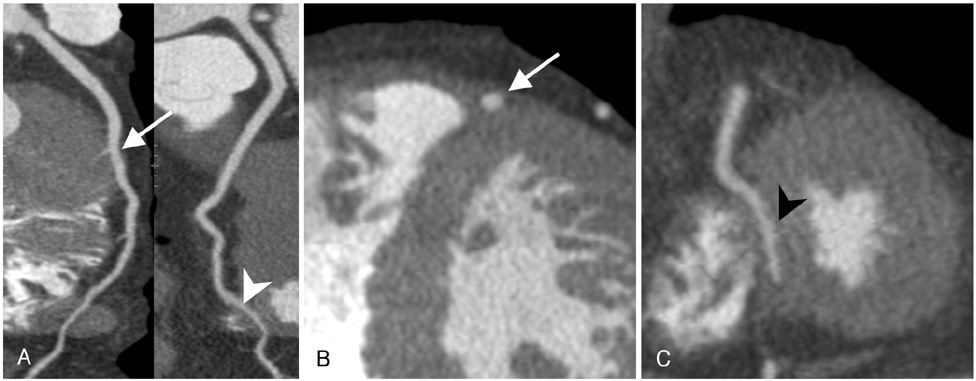
Fig. 5 A 46-year-old man presented with intermittent chest pain. (A) Curved MPR and (B and C) short-axis MIP images show two MBs in the mid-segment (arrows) and distal segment (arrowheads) of the LAD. MPR: multiplanar reconstruction, MIP: maximum intensity projection, MB: myocardial bridging, LAD: left anterior descending coronary artery.

Fig. 6 A 50-year-old man presented with atypical chest pain. (A) Axial MIP and (B) curved MPR images show a superficial MB segment in the mid-LAD (arrows). MIP: maximum intensity projection, MPR: multiplanar reconstruction, MB: myocardial bridging, LAD: left anterior descending coronary artery.

Fig. 7 A 73-year-old man presented with atypical chest pain. A and B: (A) short-axis MIP and (B) curved MPR images show a deep MB segment in the mid-LAD (arrows). C: VR image clearly demonstrates a deep MB (arrow) in the mid-LAD. MPR: multiplanar reconstruction, MIP: maximum intensity projection, MB: myocardial bridging, LAD: left anterior descending coronary artery, VR: volume-rendered.

Fig. 8 A 54-year-old man presented with atypical chest pain. (A) Axial MIP and (B) curved MPR images show a "right ventricular" type of MB segment in the mid-LAD (arrows). MPR: multiplanar reconstruction, MIP: maximum intensity projection, MB: myocardial bridging, LAD: left anterior descending coronary artery.
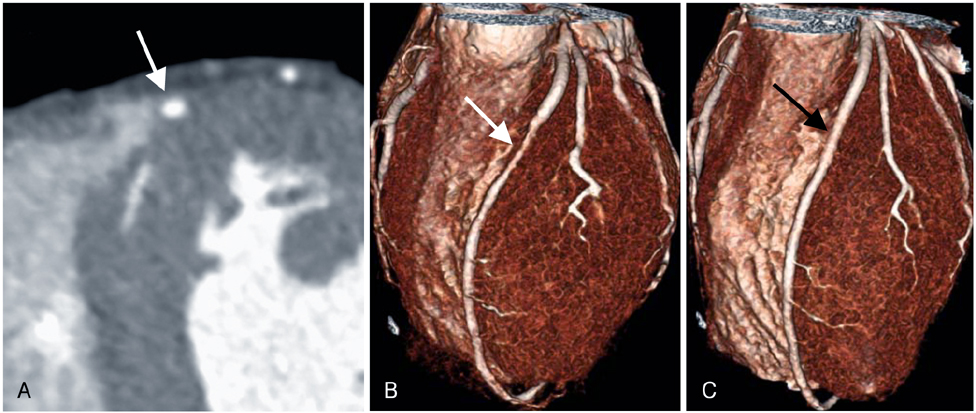
Fig. 9 Phasic luminal change in the MB using dual-source CT in a 22-year-old man with angina. A: short-axis MIP image shows a deep MB over the mid-segment of the LAD (arrow). B and C: systolic and diastolic VR images show that the lumen of the middle LAD (arrows) is compressed by myocardial contraction in the systolic phase (B), but recovers its normal diameter in the diastolic phase (C), a phenomenon known as the "milking effect". MIP: maximum intensity projection, MB: myocardial bridging, LAD: left anterior descending coronary artery, VR: volume-rendered.
Reference
-
1. Mohlenkamp S, Hort W, Ge J, Erbel R. Update on myocardial bridging. Circulation. 2002. 106:2616–2622.2. Alegria JR, Herrmann J, Holmes DR Jr, Lerman A, Rihal CS. Myocardial bridging. Eur Heart J. 2005. 26:1159–1168.3. Noble J, Bourassa MG, Petitclerc R, Dyrda I. Myocardial bridging and milking effect of the left anterior descending coronary artery: normal variant or obstruction? Am J Cardiol. 1976. 37:993–999.4. Rossi L, Dander B, Nidasio GP, et al. Myocardial bridges and ischemic heart disease. Eur Heart J. 1980. 1:239–245.5. Ferreira AG Jr, Trotter SE, Konig B Jr, Decourt LV, Fox K, Olsen EG. Myocardial bridges morphological and functional aspects. Br Heart J. 1991. 66:364–367.6. Kramer JR, Kitazume H, Proudfit WL, Sones FM Jr. Clinical significance of isolated coronary bridges: benign and frequent condition involving the left anterior descending artery. Am Heart J. 1982. 103:283–288.7. Uhm JS, Park CS, Kim TS, et al. A case of acute myocardial infarction caused by coronary thrombus associated with a myocardial bridge and slow coronary flow. Korean Circ J. 2005. 35:639–642.8. Lee JH, Bae Y, Lee HS, et al. A case of myocardial infarction in a patient with myocardial bridge and atrial fibrillation. Korean Circ J. 2004. 34:319–322.9. Kim IW, Jeung SM, Won TK, et al. Clinical observation of myocardial bridge. Korean Circ J. 2001. 31:637–644.10. Amoroso G, Battolla L, Gemignani C, et al. Myocardial bridging on left anterior descending coronary artery evaluated by multidetector computed tomography. Int J Cardiol. 2004. 95:335–337.11. Goitein O, Lacomis JM. Myocardial bridging: noninvasive diagnosis with multidetector CT. J Comput Assist Tomogr. 2005. 29:238–240.12. Ko SM, Kim KS. Multidetector-row CT coronary angiographic finding of myocardial bridging. Br J Radiol. 2007. 80:e196–e200.13. Kantarci M, Duran C, Durur I, et al. Detection of myocardial bridging with ECG-gated MDCT and multiplanar reconstruction. AJR Am J Roentgenol. 2006. 186:6 suppl 2. S391–S394.14. Zeina AR, Odeh M, Blinder J, Rosenschein U, Barmeir E. Myocardial bridge: evaluation on MDCT. AJR Am J Roentgenol. 2007. 188:1069–1073.15. Konen E, Goitein O, Sternik L, Eshet Y, Shemesh J, Di Segni E. The prevalence and anatomical patterns of intramuscular coronary arteries. J Am Coll Cardiol. 2007. 49:587–593.16. Kawawa Y, Ishikawa Y, Gomi T, et al. Detection of myocardial bridge and evaluation of its anatomical properties by coronary multislice spiral computed tomography. Eur J Radiol. 2007. 61:130–138.17. Ko SM, Choi JS, Nam CW, Hur SH. Incidence and clinical significance of myocardial bridging with ECG-gated 16-row MDCT coronary angiography. Int J Cardiovasc Imaging. 2008. 24:445–452.18. Leschka S, Koepfli P, Husmann L, et al. Myocardial bridging: depiction rate and morphology at CT coronary angiography: comparison with conventional coronary angiography. Radiology. 2008. 246:754–762.19. Hazirolan T, Canyigit M, Karcaaltincaba M, et al. Myocardial bridging on MDCT. AJR Am J Roentgenol. 2007. 188:1074–1080.20. Konen E, Goitein O, Di Segni E. Myocardial bridging, a common anatomical variant rather than a congenital anomaly. Semin Ultrasound CT MR. 2008. 29:195–203.21. Lu GM, Zhang LJ, Guo H, Huang W, Merges RD. Comparison of myocardial bridging by dual-source CT with conventional coronary angiography. Circ J. 2008. 72:1079–1085.22. Sorajja P, Ommen SR, Nishimura RA, Gersh BJ, Tajik AJ, Holmes DR. Myocardial bridging in adult patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2003. 42:889–894.23. Wymore P, Yedlicka JW, Garcia-Medina V, et al. The incidence of myocardial bridges in heart transplants. Cardiovasc Intervent Radiol. 1989. 12:202–206.24. Kopp AF, Schroeder S, Kuetner A, et al. Non-invasive coronary angiography with high resolution multidetector-row computed tomography: results in 102 patients. Eur Heart J. 2002. 23:1714–1725.25. Schoenhagen P, Halliburton SS, Stillman AE, et al. Noninvasive imaging of coronary arteries: current and future role of multi-detector row CT. Radiology. 2004. 232:7–17.26. Ochsner JL, Mills NL. Surgical management of diseased intracavitary coronary arteries. Ann Thorac Surg. 1984. 38:356–362.27. Ge J, Jeremias A, Rupp A, et al. New signs characteristic of myocardial bridging demonstrated by intracoronary ultrasound and Doppler. Eur Heart J. 1999. 20:1707–1716.28. Ge J, Erbel R, Gorge G, Haude M, Meyer J. High wall shear stress proximal to myocardial bridging and atherosclerosis: intracoronary ultrasound and pressure measurements. Br Heart J. 1995. 73:462–465.29. Ng E, Jilaihawi H, Gershlick AH. Symptomatic myocardial bridging: a niche indication for drug-eluting stents? Int J Cardiol. 2005. 99:463–464.30. Choi SH, Shim SJ, Byun KH, Choi DH, Shim WH. A case of coronary stenting in the management of myocardial ischemia caused by myocardial bridging. Korean Circ J. 2001. 31:940–944.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Correlation Between Functional Myocardial Perfusion Imaging and Anatomical Cardiac CT in a Case of Myocardial Bridging
- A Case of Q Wave Acute Myocardial Infarction in Patients with Myocardial Bridging Caused by Fibrous Band
- Coronary Flow Velocity Pattern in Patients with Myocardial Bridging of Coronary Artery
- A Case of Non-Q Myocardial Infaction in a Patient with Myocardial Bridging
- Coronary Artery Perforation Following Implantation of a Drug-Eluting Stent Rescued by Deployment of a Covered Stent in Symptomatic Myocardial Bridging
