Simvastatin, Sildenafil and Their Combination in Monocrotaline Induced Pulmonary Arterial Hypertension
- Affiliations
-
- 1Department of Pediatrics, Dongguk University School of Medicine, Gyeongju, Korea. lds117@dongguk.ac.kr
- 2Department of Physiology, Dongguk University School of Medicine, Gyeongju, Korea.
- 3Department of Anatomy, Dongguk University School of Medicine, Gyeongju, Korea.
- KMID: 2225165
- DOI: http://doi.org/10.4070/kcj.2010.40.12.659
Abstract
- BACKGROUND AND OBJECTIVES
Pulmonary arterial hypertension (PAH) is a life threatening disease characterized by progressive pulmonary arterial occlusion which may ultimately result in death. Currently, the available treatments are diverse, but no therapy alone can reverse the disease process although they may have some clinical benefits. This study was designed to investigate single and combination therapy of simvastatin and sildenafil, which have different mechanisms of action, in monocrotaline (MCT)-induced PAH. METERIALS AND METHODS: Rats were randomized to receive saline (control, n=8) or MCT treatment (n=32). MCT treated rats were randomized to vehicle, simvastatin (2 mg/kg/day), sildenafil (25 mg/kg/day) and a combination simvastatin and sildenafil (n=8, respectively). Three weeks later, hemodynamic study and histologic changes of pulmonary arterioles were measured. Proliferating cell nuclear antigen (PCNA) as well as Western blot for endothelial nitric oxide synthase (eNOS) were performed.
RESULTS
Systolic right ventricular pressure was significantly decreased in monotherapy groups (simvastatin and sildenafil) and the combination group compared to MCT group (p<0.05). Right ventricular hypertrophy and medial wall thickness of pulmonary arterioles were significantly attenuated with sole and combination therapy (p<0.05). However, combination therapy did not confer additive benefits over monotherapy. Altered PCNA or eNOS in lung tissue was normalized by either monotherapy or combination therapy.
CONCLUSION
The results suggest that either simvastatin or sildenafil has the therapeutic potential in MCT-induced PAH, although combination therapy of these two drugs has failed to show greater benefits in the study.
MeSH Terms
-
Animals
Arterioles
Blotting, Western
Hemodynamics
Hypertension
Hypertension, Pulmonary
Hypertrophy, Right Ventricular
Lung
Monocrotaline
Nitric Oxide Synthase Type III
Piperazines
Proliferating Cell Nuclear Antigen
Pulmonary Circulation
Purines
Rats
Simvastatin
Sulfones
Ventricular Pressure
Sildenafil Citrate
Hypertension, Pulmonary
Monocrotaline
Nitric Oxide Synthase Type III
Piperazines
Proliferating Cell Nuclear Antigen
Purines
Simvastatin
Sulfones
Figure
-
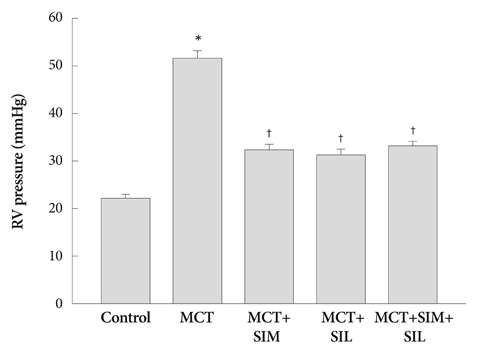
Fig. 1 Right systolic ventricle pressure. Simvastatin (SIM), sildenafil (SIL) and combination therapy (SIM+SIL) prevents the development of pulmonary arterial hypertension in monocrotaline (MCT) treated rats. However, combination therapy does not show additive effects over monotherapy. Values are expressed as mean±SD. *p<0.05 vs. control, †p<0.05 vs. MCT. RV: right ventricle.

Fig. 2 Ratio of the right ventricle (RV) to left ventricle (LV) plus septum weight. Monocrotaline (MCT)-induced RV hypertrophy was attenuated after simvastatin (SIM), sildenafil (SIL) and combination therapy (SIM+SIL). However, combination therapy did not show additional additive effects over monotherapy. Values are expressed as mean±SD. *p<0.05 vs. control, †p<0.05 vs. MCT.

Fig. 3 Medial wall thickness of pulmonary arterioles. Thickened medial wall in monocrotaline (MCT) treatment group was significantly reduced in simvastatin (SIM), sildenafil (SIL) and combination therapy (SIM+SIL). However, combination therapy did not show additional additive effects over monotherapy. Values are expressed as mean±SD. *p<0.05 vs. control, †p<0.05 vs. MCT.
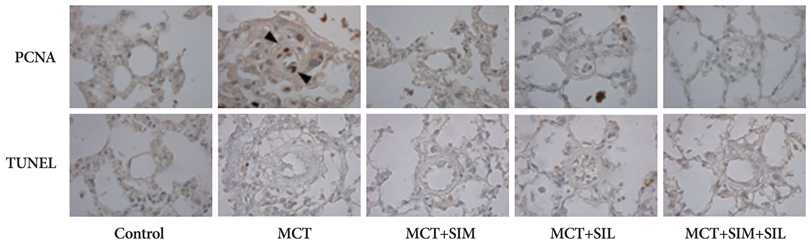
Fig. 4 Immunohistochemical stains of proliferating cell nuclear antigen (PCNA) and terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL). Monocrotaline (MCT)-induced pulmonary hypertension showed prominent smooth muscle cell proliferation of the pulmonary artery. Simvastatin (SIM), sildenafil (SIL) and combination therapy (SIM+SIL) reduced cellular proliferation. TUNEL positive cells were not evident in all groups. Arrowheads, PCNA-positive cells.
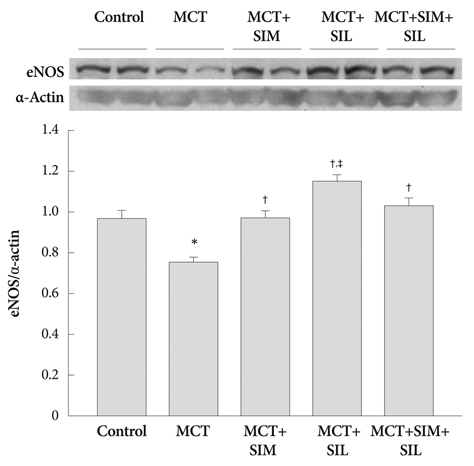
Fig. 5 Western blots for eNOS in the lung. Expression of lung eNOS was significantly diminished in the monocrotaline (MCT)-induced pulmonary hypertension. However, eNOS expression was normalized to the control level by simvastatin (SIM) and sildenafil (SIL) treatment. However, combination therapy (SIM+SIL) did not show additional additive effects over monotherapy. Values are expressed as mean±SD. *p<0.05 vs. control, †p<0.05 vs. MCT, ‡p<0.05 vs. SIM and combination. eNOS: endothelial nitric oxide synthase.
Reference
-
1. Humbert M, Morrell NW, Archer SL, et al. Cellular and molecular pathobiology of pulmonary arterial hypertension. J Am Coll Cardiol. 2004. 43:12 Suppl S. 13S–24S.2. Martin KB, Klinger JR, Rounds SI. Pulmonary arterial hypertension: new insights and new hope. Respirology. 2006. 11:6–17.3. Lee WS, Kim KH, Jeong DH, et al. Clinical characteristics and prognostic factors of patients with severe pulmonary hypertension. Korean Circ J. 2007. 37:265–270.4. Lee SH, Rubin LJ. Current treatment strategies for pulmonary arterial hypertension. J Intern Med. 2005. 258:199–215.5. Humbert M, Sitbon O, Simmoneau G. Treatment of pulmonary arterial hypertension. N Engl J Med. 2004. 351:1425–1436.6. Corsini A, Bellosta S, Baetta R, Fumagalli R, Paoletti R, Bernini F. New insights into the pharmacodynamic and pharmacokinetic properties of statins. Pharmacol Ther. 1999. 84:413–428.7. Hu H, Sung A, Zhao G, et al. Simvastatin enhances bone morphogenetic protein receptor type II expression. Biochem Biophys Res Commun. 2006. 339:59–64.8. Girgis RE, Li D, Zhan X, et al. Attenuation of chronic hypoxic pulmonary hypertension by simvastatin. Am J Physiol Heart Circ Physiol. 2003. 285:H938–H945.9. Nishimura T, Vaszar LT, Faul JL, et al. Simvastatin rescues rats from fatal pulmonary hypertension by inducing apoptosis of neointimal smooth muscle cells. Circulation. 2003. 108:1640–1645.10. Taraseviciene-Stewart L, Scerbavicius R, Choe KH, et al. Simvastatin causes endothelial cell apoptosis and attenuates severe pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol. 2006. 291:L668–L676.11. Sebkhi A, Strange JW, Phillips SC, Wharton J, Wilkins MR. Phosphodiesterase type 5 as a target for the treatment of hypoxia-induced pulmonary hypertension. Circulation. 2003. 107:3230–3235.12. Schermuly RT, Kreisselmeier KP, Ghofrani HA, et al. Chronic sildenafil treatment inhibits monocrotaline-induced pulmonary hypertension in rats. Am J Respir Crit Care Med. 2004. 169:39–45.13. Kothari SS, Duggal B. Chronic oral sildenafil therapy in severe pulmonary artery hypertension. Indian Heart J. 2002. 54:404–409.14. Sastry BK, Narasimhan C, Reddy NK, Raju BS. Clinical efficacy of sildenafil in primary pulmonary hypertension: a randomized, placebo-controlled, double-blind, crossover study. J Am Coll Cardiol. 2004. 43:1149–1153.15. Wilkins MR, Paul GA, Strange JW, et al. Sildenafil versus endothelin receptor antagonist for pulmonary hypertension (SERAPH) study. Am J Respir Crit Care Med. 2005. 171:1292–1297.16. Galiè N, Ghofrani HA, Torbicki A, et al. Sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med. 2005. 353:2148–2157.17. Takemoto M, Liao JK. Pleiotropic effects of 3-hydroxy-3-methylglutaryl coenzyme a reductase inhibitors. Arterioscler Thromb Vasc Biol. 2001. 21:1712–1719.18. Laufs U, Fata VL, Liao JK. Inhibition of 3-hydroxy-3-methylglutaryl (HMG)-CoA reductase blocks hypoxia-mediated down-regulation of endothelial nitric oxide synthase. J Biol Chem. 1997. 272:31725–31729.19. Son JW, Koh KK, You SM, et al. Effects of simvastatin alone or combined with ramipril on nitric oxide bioactivity and inflammation markers in hypercholesterolemic patients. Korean Circ J. 2003. 33:1053–1059.20. Girgis RE, Mozammel S, Champion HC, et al. Regression of chronic hypoxic pulmonary hypertension by simvastatin. Am J Physiol Lung Cell Mol Physiol. 2007. 292:L1105–L1110.21. Kim MY, Kim YK, Jung YW, Kim WT, Kwon TH, Lee DS. The protective effect of simvastatin on monocrotaline-induced pulmonary hypertension in rats. Korean Circ J. 2008. 38:313–319.22. Kao PN. Simvastatin treatment of pulmonary hypertension: an observational case series. Chest. 2005. 127:1446–1452.23. Hoeper MM, Markevych I, Spiekerkoetter E, Welte T, Niedermeyer J. Goal-oriented treatment and combination therapy for pulmonary arterial hypertension. J Eur Respir J. 2005. 26:858–863.24. Badesch DB, Abman SH, Simonneau G, Rubin LJ, McLaughlin VV. Medical therapy for pulmonary arterial hypertension: updated ACCP evidence-based clinical practice guidelines. Chest. 2007. 131:1917–1928.25. Satoh M, Satoh A. 3-Hydroxy-3-methylglutaryl (HMG)-COA reductase inhibitors and phosphodiesterase type V inhibitors attenuate right ventricular pressure and remodeling in a rat model of pulmonary hypertension. J Pharm Pharm Sci. 2009. 11:118s–130s.26. Liu H, Liu ZY, Guan Q. Oral sildenafil prevents and reverses the development of pulmonary hypertension in monocrotaline-treated rats. Interact Cardiovasc Thorac Surg. 2007. 6:608–613.27. Zhao L, Sebkhi A, Ali O, et al. Simvastatin and sildenafil combine to attenuate pulmonary hypertension. Eur Respir J. 2009. 34:948–957.28. Kuang T, Wang J, Pang B, et al. Combination of sildenafil and simvastatin ameliorates monocrotaline-induced pulmonary hypertension in rats. Pulm Pharmacol Ther. 2010. 23:456–464.29. McMurtry MS, Bonnet S, Michelakis ED, Bonnet S, Haromy A, Archer SL. Statin therapy, alone or with rapamycin, does not reverse monocrotaline pulmonary arterial hypertension: the rapamcyin-atorvastatin-simvastatin study. Am J Physiol Lung Cell Mol Physiol. 2007. 293:L933–L940.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Microarray Analysis in Pulmonary Hypertensive Rat Heart after Simvastatin Treatment
- Changes of Pulmonary Pathology and Gene Expressions After Simvastatin Treatment in the Monocrotaline-Induced Pulmonary Hypertension Rat Model
- Diagnosis and treatment of idiopathic pulmonary arterial hypertension
- The Protective Effect of Simvastatin on Monocrotaline-Induced Pulmonary Hypertension in Rats
- The effect of sildenafil on right ventricular remodeling in a rat model of monocrotaline-induced right ventricular failure
