Korean Circ J.
2011 Mar;41(3):156-159. 10.4070/kcj.2011.41.3.156.
Aortic Dissection and Rupture in a Child
- Affiliations
-
- 1Department of Pediatric Cardiology, Kwandong University Myongji Hospital Cardiovascular Center, Goyang, Korea. lucyeun@gmail.com
- 2Department of Adult Cardiology, Kwandong University Myongji Hospital Cardiovascular Center, Goyang, Korea.
- KMID: 2225131
- DOI: http://doi.org/10.4070/kcj.2011.41.3.156
Abstract
- After developing sudden severe chest pain, an 11-year-old boy presented to the emergency room with chest pain and palpitations and was unable to stand up. The sudden onset of chest pain was first reported while swimming at school about 30 minutes prior to presentation. Arterial blood pressure (BP) was 150/90 mmHg, heart rate was 120/minute, and the chest pain was combined with shortness of breath and diaphoresis. During the evaluation in the emergency room, the chest pain worsened and abdominal pain developed. An aortic dissection was suspected and a chest and abdomen CT was obtained. The diagnosis of aortic dissection type B was established by CT imaging. The patient went to surgery immediately with BP control. He died prior to surgery due to aortic rupture. Here we present this rare case of aortic dissection type B with rupture, reported in an 11-year-old Korean child.
Keyword
MeSH Terms
Figure
-
Fig. 1 The chest X-ray was normal on admission.
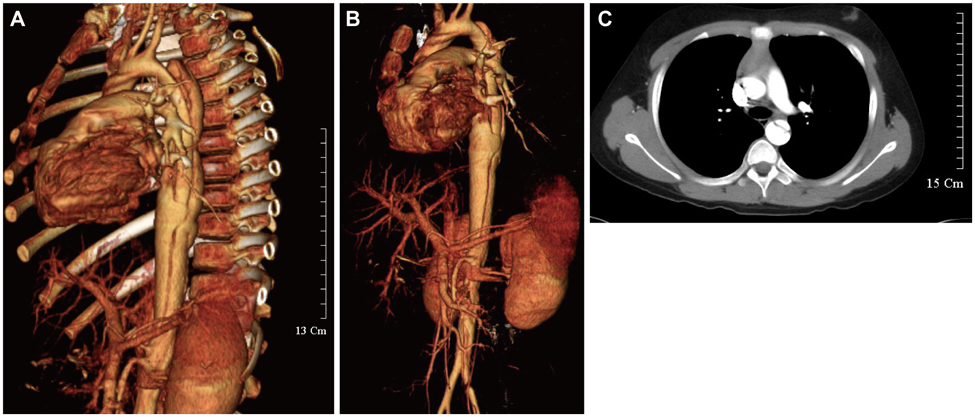
Fig. 2 Multi-detector CT image of type B aortic dissection. A: entry (arrow) and reentry (arrow) tears. B: image illustrates the extension of dissection through the left iliac artery. C: focal short segment of severe stenosis of left iliac artery was noted due to the extension of the dissection.
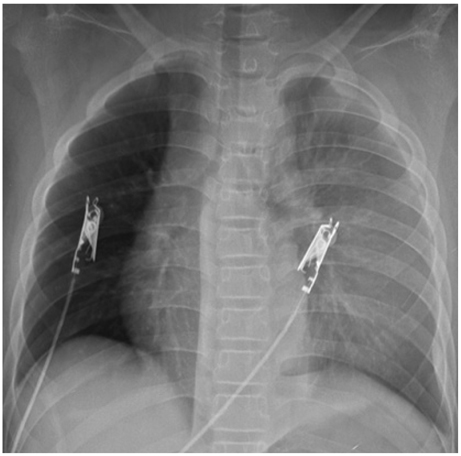
Fig. 3 The final chest X-ray turned out to show total haziness of left thorax.
Reference
-
1. Fikar CR, Fikar R. Aortic dissection in childhood and adolescence: an analysis of occurrence over a 10-year interval in New York State. Clin Cardiol. 2009. 32:E23–E26.2. Cooper DR, Lucke WC, Moseson DL. Aortic dissection in adolescence. Am Fam Physician. 1986. 34:137–142.3. Horwitz AE, Benz-Bohm G, Heuser L, Crespo E, Dalichau H. Aortic dissection in childhood: occurrence and diagnostic procedure. Monatsschr Kinderheilkd. 1986. 134:28–31.4. Fikar CR, Koch S. Etiologic factors of acute aortic dissection in children and young adults. Clin Pediatr (Phila). 2000. 39:71–80.5. Fikar CR, Amrhein JA, Harris JP, Lewis ER. Dissecting aortic aneurysm in childhood and adolescence: case report and literature review. Clin Pediatr (Phila). 1981. 20:578–583.6. Teien D, Finley JP, Murphy DA, Lacson A, Longhi J, Gillis DA. Idiopathic dilatation of the aorta with dissection in a family without Marfan syndrome. Acta Paediatr Scand. 1991. 80:1246–1249.7. Mitsnefes MM. Hypertension in children and adolescents. Pediatr Clin North Am. 2006. 53:493–512.8. Hatzaras IS, Bible JE, Koullias GJ, Tranquilli M, Singh M, Elefteriades JA. Role of exertion or emotion as inciting events for acute aortic dissection. Am J Cardiol. 2007. 100:1470–1472.9. Edwin F, Aniteye EA, Sereboe L, Frimpong-Boateng K. Acute aortic dissection in the young: distinguishing precipitating from predisposing factors. Interact Cardiovasc Thorac Surg. 2009. 9:368.10. Gray J, McCaw T, McGovern S. Spontaneous chest pain in a 14-year-old boy. Eur J Emerg Med. 2005. 12:253–254.11. Rizzoli G, Scalia D, Casarotto D, Tiso E. Aortic dissection type A versus type B: a different post-surgical death hazard? Eur J Cardiothorac Surg. 1997. 12:202–208.12. Schor JS, Yerlioglu ME, Galla JD, Lansman SL, Ergin MA, Griepp RB. Selective management of acute type B aortic dissection: long-term follow-up. Ann Thorac Surg. 1996. 61:1339–1341.13. Hashimoto A, Kimata S, Hosoda S. Acute aortic dissection: a comparison between the results of medical and surgical treatments. Jpn Circ J. 1991. 55:821–823.14. Cho SH, Sung K, Park KH, et al. Midterm results of aortic arch replacement in a Stanford type A aortic dissection with an intimal tear in the aortic arch. Korean Circ J. 2009. 39:270–274.15. Qureshi SA. Use of covered stents to treat coarctation of the aorta. Korean Circ J. 2009. 39:261–263.16. Park SH, Park HS, Lee JH, et al. A case of coronary artery dissection after aortic replacement in acute type A aortic dissection. Korean Circ J. 2009. 39:428–423.17. Lee S, Kim W, Hwang SH, et al. The relationship of inflammatory reaction with the mortality of type B acute aortic syndrome. Korean Circ J. 2006. 36:387–392.18. Kang WC, Joung BY, Ko YG, et al. Favorable outcome of endovascular stent-graft implantation for Stanford type B aortic dissection. Korean Circ J. 2003. 33:457–464.19. Fishbein MC. Cardiac disease and risk of sudden death in the young the burden of the phenomenon. Cardiovasc Pathol. 2009. [Epub ahead of print].20. DeSanctis RW, Doroghazi RM, Austen WG, Buckley MJ. Aortic dissection. N Engl J Med. 1987. 317:1060–1067.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Retrograde Aortic Dissection after Thoracic Endovascular Aortic Repair for Descending Aorta: 2 case reports
- A Case of Kommerell's Diverticulum with Aortic Dissection
- A Case of Term Cesarean Delivery in Patient with Ascending Aortic Aneurysm : Complicated by Rupture of Aortic Dissection
- Current Status of Acute Aortic Disease Treatment
- Classification of Aneurysmal Aortitides: By CT Findings
