Korean Circ J.
2012 Nov;42(11):741-746. 10.4070/kcj.2012.42.11.741.
Fenofibrate Reduces C-Reactive Protein Levels in Hypertriglyceridemic Patients With High Risks for Cardiovascular Diseases
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, College of Medicine, Chung-Ang University, Seoul, Korea. cjkim@cau.ac.kr
- KMID: 2224973
- DOI: http://doi.org/10.4070/kcj.2012.42.11.741
Abstract
- BACKGROUND AND OBJECTIVES
The effects of fenofibrate on C-reactive protein (CRP) are under debate. We investigated the effect of fenofibrate on CRP levels and the variables determining changes.
SUBJECTS AND METHODS
This case-control study enrolled 280 hypertriglyceridemic patients who were managed either with 200 mg of fenofibrate (Fenofibrate group, n=140) or with standard treatment (comparison group, n=140). CRP levels were measured before and after management for 2 months.
RESULTS
CRP levels decreased in both the fenofibrate (p=0.003) and comparison (p=0.048) groups. Changes in CRP levels were not significantly different between the two groups (p=0.27) and were negatively associated with baseline CRP levels (r=-0.47, p<0.001). In patients with a baseline CRP level > or =1 mg/L, CRP levels also decreased in both groups (p=0.000 and p=0.001 respectively), however, more in the fenofibrate group than in the comparison group (p=0.025). The reduction of CRP was associated with higher baseline CRP levels (r=-0.29, p=0.001), lower body mass index (BMI, r=0.23, p=0.007), and fenofibrate therapy (r=0.19, p=0.025). CRP levels decreased more in the fenofibrate group than in the comparison group in patients with a BMI < or =26 kg/m2 with borderline significance (-1.21+/-1.82 mg/L vs. -0.89+/-1.92 mg/L, p=0.097). In patients with a high density lipoprotein-cholesterol level <40 mg/dL, CRP levels were reduced only in the fenofibrate group (p=0.006).
CONCLUSION
Fenofibrate reduced CRP levels in hypertriglyceridemic patients with high CRP and/or low high density lipoprotein-cholesterol levels and without severe overweight. This finding suggests that fenofibrate may have an anti-inflammatory effect in selected patients.
Keyword
MeSH Terms
Figure
-

Fig. 1 The relation between baseline C-reactive protein (CRP) levels and changes in CRP levels in all patients (A), patients with a baseline CRP level ≥1 mg/L (B), and patients with a baseline CRP level <1 mg/L (C).
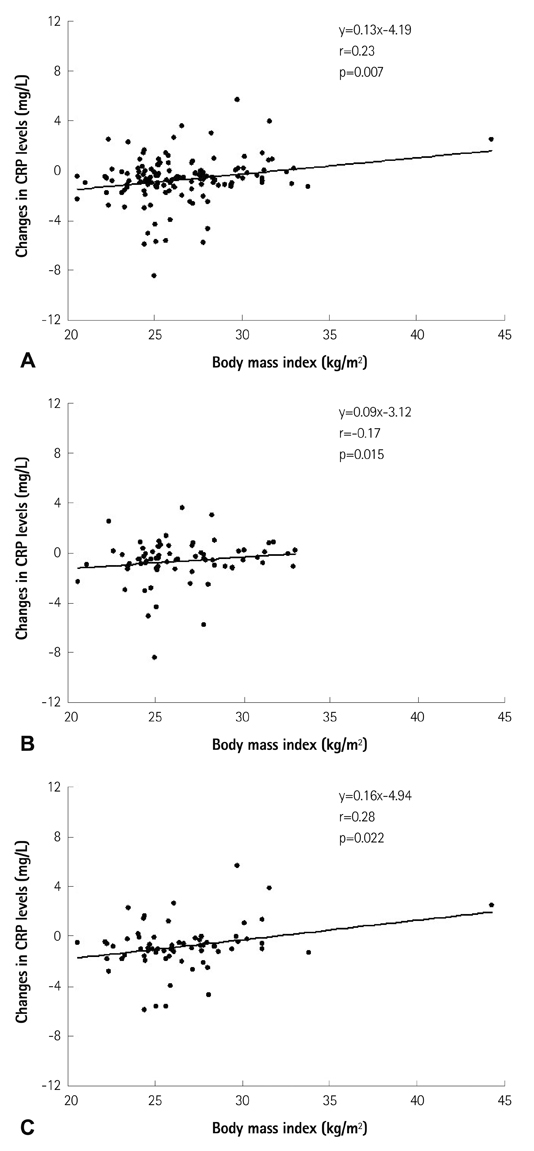
Fig. 2 The relation between changes in C-reactive protein (CRP) levels and body mass index in patients with a baseline CRP level ≥1 mg/L. A: all patients. B: the comparison group. C: the fenofibrate group.
Cited by 1 articles
-
Role of Fenofibrate Use in Dyslipidemia and Related Comorbidities in the Asian Population: A Narrative Review
Chaicharn Deerochanawong, Sin Gon Kim, Yu-Cheng Chang
Diabetes Metab J. 2024;48(2):184-195. doi: 10.4093/dmj.2023.0168.
Reference
-
1. Shah A, Rader DJ, Millar JS. The effect of PPAR-alpha agonism on apolipoprotein metabolism in humans. Atherosclerosis. 2010. 210:35–40.2. Frick MH, Elo O, Haapa K, Heinonen OP, et al. Helsinki Heart Study: primary-prevention trial with gemfibrozil in middle-aged men with dyslipidemia. Safety of treatment, changes in risk factors, and incidence of coronary heart disease. N Engl J Med. 1987. 317:1237–1245.3. Rubins HB, Robins SJ, Collins D, et al. Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial Study Group. Gemfibrozil for the secondary prevention of coronary heart disease in men with low levels of high-density lipoprotein cholesterol. N Engl J Med. 1999. 341:410–418.4. Secondary prevention by raising HDL cholesterol and reducing triglycerides in patients with coronary artery disease: the Bezafibrate Infarction Prevention (BIP) study. Circulation. 2000. 102:21–27.5. Keech A, Simes RJ, Barter P, et al. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): randomised controlled trial. Lancet. 2005. 366:1849–1861.6. ACCORD Study Group. Ginsberg HN, Elam MB, et al. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med. 2010. 362:1563–1574.7. Ross R. Atherosclerosis--an inflammatory disease. N Engl J Med. 1999. 340:115–126.8. Ridker PM. Clinical application of C-reactive protein for cardiovascular disease detection and prevention. Circulation. 2003. 107:363–369.9. Staels B, Koenig W, Habib A, et al. Activation of human aortic smooth-muscle cells is inhibited by PPARalpha but not by PPARgamma activators. Nature. 1998. 393:790–793.10. Malik J, Melenovsky V, Wichterle D, et al. Both fenofibrate and atorvastatin improve vascular reactivity in combined hyperlipidaemia (fenofibrate versus atorvastatin trial--FAT). Cardiovasc Res. 2001. 52:290–298.11. Wu TJ, Ou HY, Chou CW, Hsiao SH, Lin CY, Kao PC. Decrease in inflammatory cardiovascular risk markers in hyperlipidemic diabetic patients treated with fenofibrate. Ann Clin Lab Sci. 2007. 37:158–166.12. Cortellaro M, Cofrancesco E, Boschetti C, et al. Effects of fluvastatin and bezafibrate combination on plasma fibrinogen, t-plasminogen activator inhibitor and C reactive protein levels in coronary artery disease patients with mixed hyperlipidaemia (FACT study). Fluvastatin Alone and in Combination Treatment. Thromb Haemost. 2000. 83:549–553.13. Gómez-Gerique JA, Ros E, Oliván J, et al. Effect of atorvastatin and bezafibrate on plasma levels of C-reactive protein in combined (mixed) hyperlipidemia. Atherosclerosis. 2002. 162:245–251.14. Wang TD, Chen WJ, Lin JW, Cheng CC, Chen MF, Lee YT. Efficacy of fenofibrate and simvastatin on endothelial function and inflammatory markers in patients with combined hyperlipidemia: relations with baseline lipid profiles. Atherosclerosis. 2003. 170:315–323.15. Hogue JC, Lamarche B, Tremblay AJ, Bergeron J, Gagné C, Couture P. Differential effect of atorvastatin and fenofibrate on plasma oxidized low-density lipoprotein, inflammation markers, and cell adhesion molecules in patients with type 2 diabetes mellitus. Metabolism. 2008. 57:380–386.16. Muhlestein JB, May HT, Jensen JR, et al. The reduction of inflammatory biomarkers by statin, fibrate, and combination therapy among diabetic patients with mixed dyslipidemia: the DIACOR (Diabetes and Combined Lipid Therapy Regimen) study. J Am Coll Cardiol. 2006. 48:396–401.17. Jonkers IJ, Mohrschladt MF, Westendorp RG, van der Laarse A, Smelt AH. Severe hypertriglyceridemia with insulin resistance is associated with systemic inflammation: reversal with bezafibrate therapy in a randomized controlled trial. Am J Med. 2002. 112:275–280.18. Farnier M, Freeman MW, Macdonell G, et al. Efficacy and safety of the coadministration of ezetimibe with fenofibrate in patients with mixed hyperlipidaemia. Eur Heart J. 2005. 26:897–905.19. Belfort R, Berria R, Cornell J, Cusi K. Fenofibrate reduces systemic inflammation markers independent of its effects on lipid and glucose metabolism in patients with the metabolic syndrome. J Clin Endocrinol Metab. 2010. 95:829–836.20. Ye P, Li JJ, Su G, Zhang C. Effects of fenofibrate on inflammatory cytokines and blood pressure in patients with hypertriglyceridemia. Clin Chim Acta. 2005. 356:229–232.21. Okopień B, Krysiak R, Kowalski J, et al. Monocyte release of tumor necrosis factor-alpha and interleukin-1beta in primary type IIa and IIb dyslipidemic patients treated with statins or fibrates. J Cardiovasc Pharmacol. 2005. 46:377–386.22. Okopień B, Krysiak R, Herman ZS. Effects of short-term fenofibrate treatment on circulating markers of inflammation and hemostasis in patients with impaired glucose tolerance. J Clin Endocrinol Metab. 2006. 91:1770–1778.23. Kim CJ. Effects of fenofibrate on C-reactive protein levels in hypertriglyceridemic patients. J Cardiovasc Pharmacol. 2006. 47:758–763.24. Haim M, Benderly M, Tanne D, et al. C-reactive protein, bezafibrate, and recurrent coronary events in patients with chronic coronary heart disease. Am Heart J. 2007. 154:1095–1101.25. Hiukka A, Westerbacka J, Leinonen ES, et al. Long-term effects of fenofibrate on carotid intima-media thickness and augmentation index in subjects with type 2 diabetes mellitus. J Am Coll Cardiol. 2008. 52:2190–2197.26. Shin HS, Sung KC, Kim BJ, et al. Effect of exercise on serum C-reactive protein. Korean Circ J. 2005. 35:533–538.27. Kim SJ, Lee KE, Lee SH, et al. Effect of fibrate on lipoprotein(a) level in hypertriglyceridemic patients. Korean Circ J. 2005. 35:30–36.28. Ridker PM, Rifai N, Pfeffer MA, et al. Cholesterol and Recurrent Events (CARE) Investigators. Inflammation, pravastatin, and the risk of coronary events after myocardial infarction in patients with average cholesterol levels. Circulation. 1998. 98:839–844.29. Shen J, Ordovas JM. Impact of genetic and environmental factors on hsCRP concentrations and response to therapeutic agents. Clin Chem. 2009. 55:256–264.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of fenofibrate on C-reactive protein levels in hypertriglyceridemic patients
- Effect of Long-term Fenofibrate Therapy on Serum Creatinine and Its Reversibility in Hypertriglyceridemic Patients with Hypertension
- Effect of Short-term Fenofibrate Therapy on Blood Creatinine Levels in Patients with Hypertriglyceridemia
- The Role and Clinical Significance of High-Sensitivity C-Reactive Protein in Cardiovascular Disease
- Control of Dyslipidemia
