Pericardial Effusion and Pericardiocentesis: Role of Echocardiography
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. hojheart@catholic.ac.kr
- KMID: 2224971
- DOI: http://doi.org/10.4070/kcj.2012.42.11.725
Abstract
- Pericardial effusion can develop from any pericardial disease, including pericarditis and several systemic disorders, such as malignancies, pulmonary tuberculosis, chronic renal failure, thyroid diseases, and autoimmune diseases. The causes of large pericardial effusion requiring invasive pericardiocentesis may vary according to the time, country, and hospital. Transthoracic echocardiography is the most important tool for diagnosis, grading, the pericardiocentesis procedure, and follow up of pericardial effusion. Cardiac tamponade is a kind of cardiogenic shock and medical emergency. Clinicians should understand the tamponade physiology, especially because it can develop without large pericardial effusion. In addition, clinicians should correlate the echocardiographic findings of tamponade, such as right ventricular collapse, right atrial collapse, and respiratory variation of mitral and tricuspid flow, with clinical signs of clinical tamponade, such as hypotension or pulsus paradoxus. Percutaneous pericardiocentesis has been the most useful procedure in many cases of large pericardial effusion, cardiac tamponade, or pericardial effusion of unknown etiology. The procedure should be performed with the guidance of echocardiography.
MeSH Terms
Figure
-

Fig. 1 Representative images of echo-free space on 2-dimensional echocardiography.
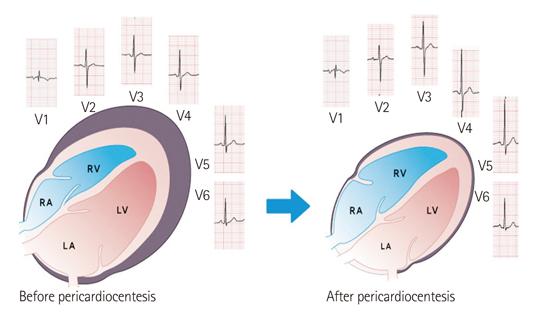
Fig. 2 Schematic showing that pericardial effusion mainly accumulates around the 2 ventricles, rather than the 2 atria; therefore, the p waves are not changed much after pericardiocentesis, compared with the Q wave (Jung HO et al. Am J Cardiol 2010;106:441 with permission).18) RA: right atrium, LA: left atrium, RV: right ventricle, LV: left ventricle.

Fig. 3 Echocardiographic grading of pericardial effusion as scanty (A), mild (B), moderate (C), and large (D).
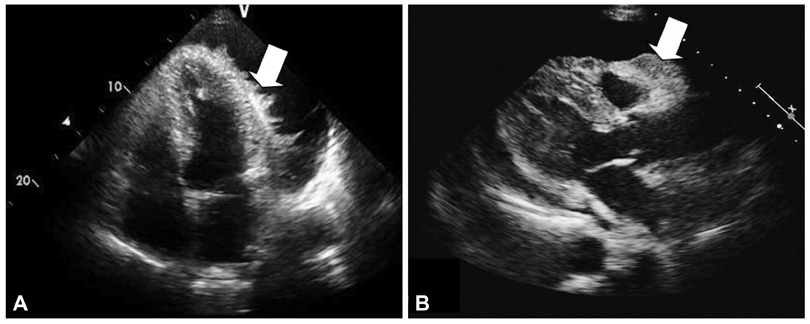
Fig. 4 Echocardiography showing abnormal masses on the epicardial surface. Final diagnoses are (A) post-operative pericarditis and (B) metastatic infiltration of lung cancer to pericardium.
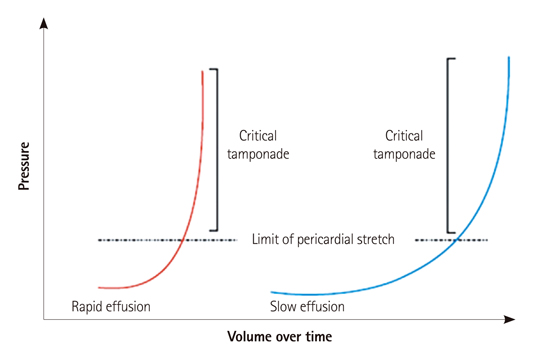
Fig. 5 Pericardial pressure-volume relationships in patients who have rapidly (left curve) and gradually (right curve) developed a pericardial effusion. In rapid accumulating effusion (left curve), even a small effusion volume can exceed the limit of parietal pericardial stretch and finally causes a steep rise in pressure. In contrast, slow accumulating effusion (right curve) requires a long time and a large volume to exceed the limit of pericardial stretch because of the activating compensatory mechanisms (Spodick DH. N Engl J Med 2003;349:685 with permission).20)
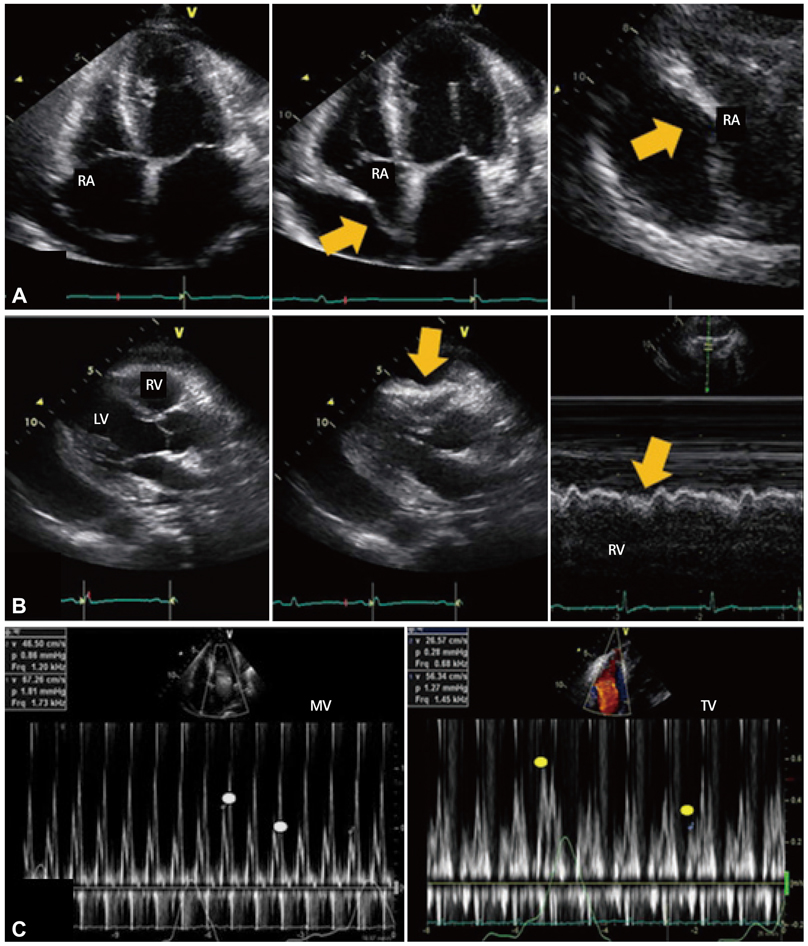
Fig. 6 Representative echocardiographic images of cardiac tamponade. A: diastolic collapse of the free wall of the right atrium from late diastole to early systole is observed on the apical 4 chamber view (middle) and magnified view (right), compared with the image of early diastole (left). B: collapse of the right ventricle in early diastole is observed on the parasternal long axis view (middle) and M-mode (right), compared with the image of systole (left). C: marked respiratory variation is observed on the transmitral (left) and transtricuspid (right) Doppler flow. RA: right atrium, RV: right ventricle, LV: left ventricle, MV: mitral valve, TV: tricuspid valve.
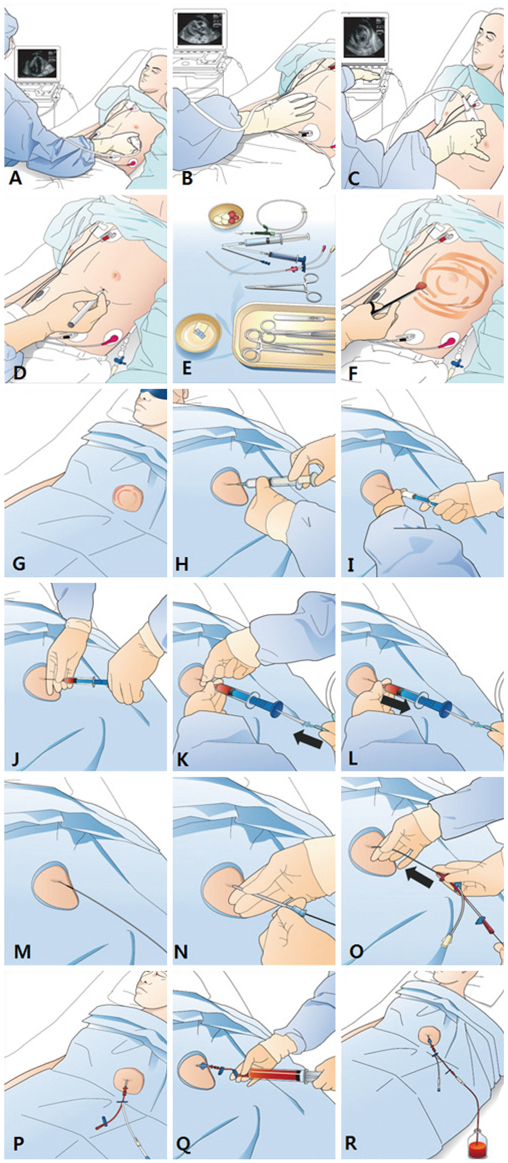
Fig. 7 Illustrations of the procedure of echocardiography guided percutaneous pericardiocentesis.
Reference
-
1. Little WC, Freeman GL. Pericardial disease. Circulation. 2006. 113:1622–1632.2. Braunwalt E. Fausi AS, Braunwalt E, Kasper DL, editors. Pericardial disease. Harrison's internal medicine. 2008. 17th ed. New York: McGraw Hill Medical;1488–1492.3. Oh JK, Seward JB, Tajik AJ. Oh JK, Seward JB, Tajik AJ, editors. Pericardial diseases. The echo manual. 2007. 3rd ed. Philadelphia: Lippincott Williams and Wilkins (Wolters Kluwers);289–292.4. Munt BI, Moss RR, Grewal J. Otto CM, editor. Pericardial disease. The practice of clinical echocardiography. 2011. 4th ed. Philadelphia: Saunders/Elservier;565–578.5. Manning WJ. Goldman L, Ausiello D, editors. Pericardial disease. Cecil Medicine. 2008. 23rd ed. Philadelphia: Saunders/Elservier;548–552.6. Sagristà-Sauleda J, Mercé AS, Soler-Soler J. Diagnosis and management of pericardial effusion. World J Cardiol. 2011. 3:135–143.7. Maisch B, Seferović PM, Ristić AD, et al. Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology. Eur Heart J. 2004. 25:587–610.8. Kil UH, Jung HO, Koh YS, et al. Prognosis of large, symptomatic pericardial effusion treated by echo-guided percutaneous pericardiocentesis. Clin Cardiol. 2008. 31:531–537.9. Cho BC, Kang SM, Kim DH, et al. Clinical and echocardiographic characteristics of pericardial effusion in patients who underwent echocardiographically guided pericardiocentesis: Yonsei Cardiovascular Center experience, 1993-2003. Yonsei Med J. 2004. 45:462–468.10. Kim DY, Park JH, Shin JD, et al. Long-term follow-up results and clinical manifestations of patients with a moderate to large amount of pericardial effusion. Korean J Med. 2008. 74:154–161.11. Tsang TS, Enriquez-Sarano M, Freeman WK, et al. Consecutive 1127 therapeutic echocardiographically guided pericardiocenteses: clinical profile, practice patterns, and outcomes spanning 21 years. Mayo Clin Proc. 2002. 77:429–436.12. Kabukcu M, Demircioglu F, Yanik E, Basarici I, Ersel F. Pericardial tamponade and large pericardial effusions: causal factors and efficacy of percutaneous catheter drainage in 50 patients. Tex Heart Inst J. 2004. 31:398–403.13. Sagristà-Sauleda J, Mercé J, Permanyer-Miralda G, Soler-Soler J. Clinical clues to the causes of large pericardial effusions. Am J Med. 2000. 109:95–101.14. Levy PY, Corey R, Berger P, et al. Etiologic diagnosis of 204 pericardial effusions. Medicine (Baltimore). 2003. 82:385–391.15. Reuter H, Burgess LJ, Doubell AF. Epidemiology of pericardial effusions at a large academic hospital in South Africa. Epidemiol Infect. 2005. 133:393–399.16. Horowitz MS, Schultz CS, Stinson EB, Harrison DC, Popp RL. Sensitivity and specificity of echocardiographic diagnosis of pericardial effusion. Circulation. 1974. 50:239–247.17. Pepi M, Muratori M. Echocardiography in the diagnosis and management of pericardial disease. J Cardiovasc Med (Hagerstown). 2006. 7:533–544.18. Jung HO, Seung KB, Madias JE. Electrocardiographic changes resulting from pericardial effusion drainage. Am J Cardiol. 2010. 106:437–441.19. Verhaert D, Gabriel RS, Johnston D, Lytle BW, Desai MY, Klein AL. The role of multimodality imaging in the management of pericardial disease. Circ Cardiovasc Imaging. 2010. 3:333–343.20. Spodick DH. Acute cardiac tamponade. N Engl J Med. 2003. 349:684–690.21. Ariyarajah V, Spodick DH. Cardiac tamponade revisited: a postmortem look at a cautionary case. Tex Heart Inst J. 2007. 34:347–351.22. Kronzon I, Cohen ML, Winer HE. Cardiac tamponade by loculated pericardial hematoma: limitations of M-mode echocardiography. J Am Coll Cardiol. 1983. 1:913–915.23. Tsang TS, Barnes ME, Hayes SN, et al. Clinical and echocardiographic characteristics of significant pericardial effusions following cardiothoracic surgery and outcomes of echo-guided pericardiocentesis for management: Mayo Clinic experience, 1979-1998. Chest. 1999. 116:322–331.24. Singh S, Wann LS, Schuchard GH, et al. Right ventricular and right atrial collapse in patients with cardiac tamponade--a combined echocardiographic and hemodynamic study. Circulation. 1984. 70:966–971.25. Gillam LD, Guyer DE, Gibson TC, King ME, Marshall JE, Weyman AE. Hydrodynamic compression of the right atrium: a new echocardiographic sign of cardiac tamponade. Circulation. 1983. 68:294–301.26. Kochar GS, Jacobs LE, Kotler MN. Right atrial compression in postoperative cardiac patients: detection by transesophageal echocardiography. J Am Coll Cardiol. 1990. 16:511–516.27. Gaffney FA, Keller AM, Peshock RM, Lin JC, Firth BG. Pathophysiologic mechanisms of cardiac tamponade and pulsus alternans shown by echocardiography. Am J Cardiol. 1984. 53:1662–1666.28. Armstrong WF, Schilt BF, Helper DJ, Dillon JC, Feigenbaum H. Diastolic collapse of the right ventricle with cardiac tamponade: an echocardiographic study. Circulation. 1982. 65:1491–1496.29. Engel PJ, Hon H, Fowler NO, Plummer S. Echocardiographic study of right ventricular wall motion in cardiac tamponade. Am J Cardiol. 1982. 50:1018–1021.30. Reydel B, Spodick DH. Frequency and significance of chamber collapses during cardiac tamponade. Am Heart J. 1990. 119:1160–1163.31. Appleton CP, Hatle LK, Popp RL. Cardiac tamponade and pericardial effusion: respiratory variation in transvalvular flow velocities studied by Doppler echocardiography. J Am Coll Cardiol. 1988. 11:1020–1030.32. Burstow DJ, Oh JK, Bailey KR, Seward JB, Tajik AJ. Cardiac tamponade: characteristic Doppler observations. Mayo Clin Proc. 1989. 64:312–324.33. Himelman RB, Kircher B, Rockey DC, Schiller NB. Inferior vena cava plethora with blunted respiratory response: a sensitive echocardiographic sign of cardiac tamponade. J Am Coll Cardiol. 1988. 12:1470–1477.34. Mercé J, Sagristà-Sauleda J, Permanyer-Miralda G, Evangelista A, Soler-Soler J. Correlation between clinical and Doppler echocardiographic findings in patients with moderate and large pericardial effusion: implications for the diagnosis of cardiac tamponade. Am Heart J. 1999. 138(4 Pt 1):759–764.35. Nagdev A, Stone MB. Point-of-care ultrasound evaluation of pericardial effusions: does this patient have cardiac tamponade? Resuscitation. 2011. 82:671–673.36. Tsang TS, Freeman WK, Barnes ME, Reeder GS, Packer DL, Seward JB. Rescue echocardiographically guided pericardiocentesis for cardiac perforation complicating catheter-based procedures. The Mayo Clinic experience. J Am Coll Cardiol. 1998. 32:1345–1350.37. Seferović PM, Ristić AD, Imazio M, et al. Management strategies in pericardial emergencies. Herz. 2006. 31:891–900.38. Lindenberger M, Kjellberg M, Karlsson E, Wranne B. Pericardiocentesis guided by 2-D echocardiography: the method of choice for treatment of pericardial effusion. J Intern Med. 2003. 253:411–417.39. Halpern DG, Argulian E, Briasoulis A, Chaudhry F, Aziz EF, Herzog E. A novel pericardial effusion scoring index to guide decision for drainage. Crit Pathw Cardiol. 2012. 11:85–88.40. Goodman A, Perera P, Mailhot T, Mandavia D. The role of bedside ultrasound in the diagnosis of pericardial effusion and cardiac tamponade. J Emerg Trauma Shock. 2012. 5:72–75.41. Loukas M, Walters A, Boon JM, Welch TP, Meiring JH, Abrahams PH. Pericardiocentesis: a clinical anatomy review. Clin Anat. 2012. 25:872–881.42. Tsang TS, Freeman WK, Sinak LJ, Seward JB. Echocardiographically guided pericardiocentesis: evolution and state-of-the-art technique. Mayo Clin Proc. 1998. 73:647–652.43. Spodick DH. Braunwald E, Zipes DP, Libby P, editors. Pericardial diseases. Heart disease. 2001. 6th ed. Philadelphia: W.B. Saunders;1823–1876.44. Allen KB, Faber LP, Warren WH, Shaar CJ. Pericardial effusion: subxiphoid pericardiostomy versus percutaneous catheter drainage. Ann Thorac Surg. 1999. 67:437–440.45. McDonald JM, Meyers BF, Guthrie TJ, Battafarano RJ, Cooper JD, Patterson GA. Comparison of open subxiphoid pericardial drainage with percutaneous catheter drainage for symptomatic pericardial effusion. Ann Thorac Surg. 2003. 76:811–815. discussion 816.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Disappearance of pericardial effusion by suspected pericardial-pleural fistulain a Miniature Schnauzer dog
- Successful Treatment of Cardiac Tamponade Associated with Umbilical Venous Catheter by Pericardiocentesis in Two Neonates: Two Case Reports
- Estimating the Volume of Pericardial Effusion by M-Mode and 2-D Echocardiographic Method
- A "Vanishing", Tuberculous, Pericardial Effusion
- Pneumopericardium: A Rare Complication of Pericardiocentesis
