An Adolescent Patient with Coarctation of Aorta Treated with Self-Expandable Nitinol Stent
- Affiliations
-
- 1Department of Pediatric Cardiology, Sejong Cardiovascular Center, Sejong General Hospital, Bucheon, Korea. wsshim01@gmail.com
- 2Department of Radiology, Sejong Cardiovascular Center, Sejong General Hospital, Bucheon, Korea.
- 3Department of Pediatric Cardiology, Samsung Medical Center, Seoul, Korea.
- KMID: 2224969
- DOI: http://doi.org/10.4070/kcj.2013.43.3.207
Abstract
- Transcatheter treatment of aortic coarctation, with balloon angioplasty or stent implantation, is now an acceptable alternative to surgical repair. However these procedures may result in complications, such as vascular wall injury and re-stenosis of the lesion. A nitinol self-expandable stent, when deployed at the coarctation site, produces low constant radial force, which may result in a gradual widening of the stenotic lesion leaving less tissue injury ('stretching rather than tearing'). For an adolescent with a native aortic coarctation, a self-expandable stent of 20 mm diameter was inserted at the discrete stenotic lesion of 5 mm diameter without previous balloon dilatation procedure. No further balloon dilatation was done immediately after the stent insertion. With the self-expandable stent only, the stenosis of the lesion was partially relieved immediately after the stent deployment. Over several months after the stent insertion, gradual further widening of the stent waist to an acceptable dimension was observed.
Keyword
MeSH Terms
Figure
-
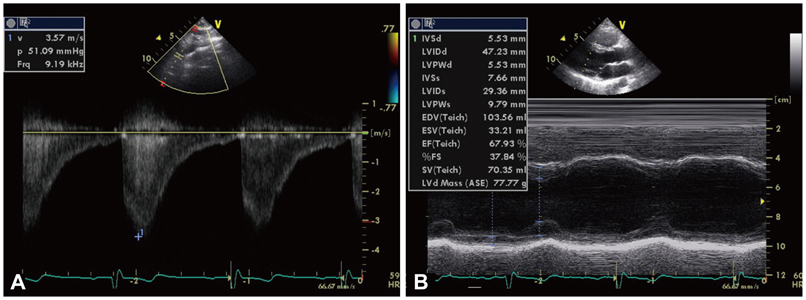
Fig. 1 Echocardiographic examination before the insertion of the stent. A: Doppler study showed a maximum pressure gradient of 50 mm Hg across the aortic coarctation. B: M-mode echocardiagram showed relatively good systolic function of left ventricle without significant muscle wall hypertrophy.

Fig. 2 Images of the aortic coarctation at the time of stent insertion. A: multi-planar reconstructed CT images before the stent insertion showed discrete narrowing at the isthmic portion of aortic arch due to posterior shelf lesion measuring 4 mm in the narrowest dimension. B: aortic angiogram before the insertion of the stent showed discrete narrowing at the isthmus of the aortic arch measuring 5 mm in the narrowest dimension. C: aortic angiogram immediately after the insertion of the self-expandable nitinol stent showed the dimension of the stent waist 8 mm.
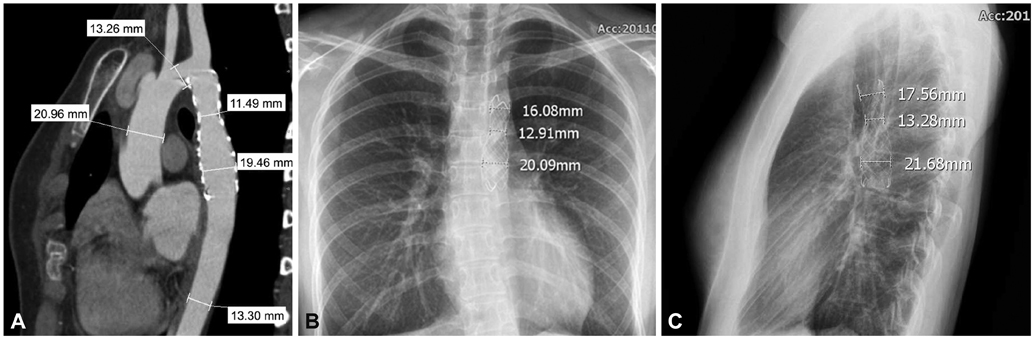
Fig. 3 Images of the aortic coarctation 3 months after the insertion of the self-expandable stent. A: multiplanar reconstructed CT images 3 months after the insertion of the self-expandable nitinol stent showed the dimension of the stent waist 11.5 mm. B and C: chest X-ray images 3 months after the insertion of the self-expandable nitinol stent showed the dimension of the stent waist 13 mm (B: anterior-posterior projection, C: lateral projection).

Fig. 4 Chest X-ray images 1 year after the insertion of the stent. Chest X ray images showed the dimension of the stent waist 14 mm. A: anterior-posterior projection. B: lateral projection.
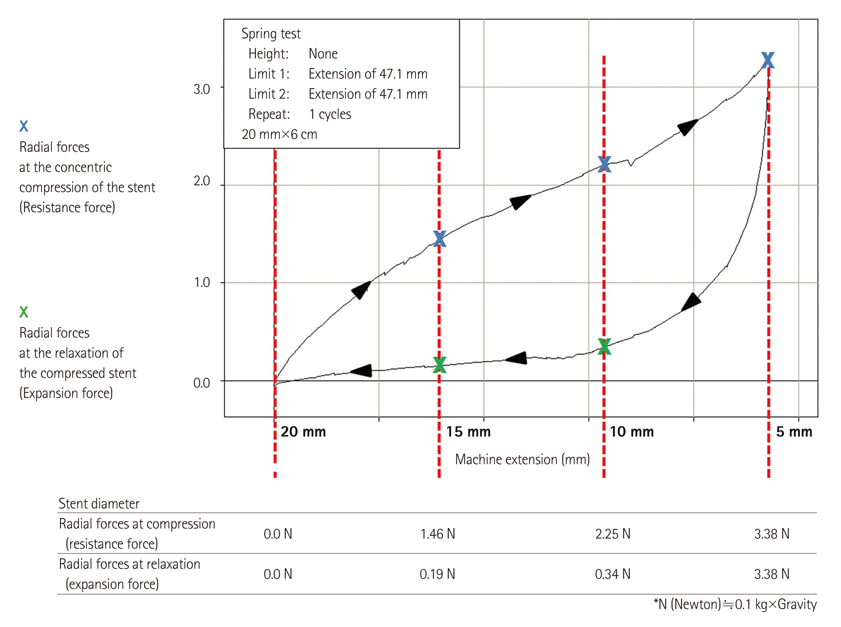
Fig. 5 In the concentric compression and relaxation experiment of the self-expandable nitinol stent (S&G Biotech, Seongnam, Korea), the radial forces of the stent were measured at varying diameters of the stent. The 20 mm diameter self-expandable stent was tightened gradually by a ringed device to the diameter of 5 mm and thereafter loosened gradually to the diameter of 20 mm. As the stent is deformed to a smaller diameter, the stronger the radial force was observed. And as the diameter of the stent increased, the radial force exerted by the stent decreased rather steeply. The resistance force of the stent measured when the concentric compression force was loaded was greater than the expansion force of the stent measured when the concentric force was unloaded (Data from S&G Biotech, Seongnam, Korea).
Reference
-
1. Chessa M, Carrozza M, Butera G, et al. Results and mid-long-term follow-up of stent implantation for native and recurrent coarctation of the aorta. Eur Heart J. 2005. 26:2728–2732.2. Kische S, Schneider H, Akin I, et al. Technique of interventional repair in adult aortic coarctation. J Vasc Surg. 2010. 51:1550–1559.3. Golden AB, Hellenbrand WE. Coarctation of the aorta: stenting in children and adults. Catheter Cardiovasc Interv. 2007. 69:289–299.4. Dyet JF, Watts WG, Ettles DF, Nicholson AA. Mechanical properties of metallic stents: how do these properties influence the choice of stent for specific lesions? Cardiovasc Intervent Radiol. 2000. 23:47–54.5. Stoeckel D, Pelton A, Duerig T. Self-expanding nitinol stents: material and design considerations. Eur Radiol. 2004. 14:292–301.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A successful stenting of the coarctation of aorta in a patient with acute pulmonary edema
- A Case Report: Implantation of Balloon-Expandable Stent for Coarctation of the Aorta, Associated with Congenital Mitral Stenosis
- Use of Covered Stents to Treat Coarctation of the Aorta
- A Dual Expandable Nitinol Stent: The Long-term Results in Patients with Malignant Gastroduodenal Strictures
- A Case of Coarctation of the Aorta Treated with Balloon Angioplasty
