A Case of Successful Bare Metal Stenting for Aortic Coarctation in an Adult
- Affiliations
-
- 1Department of Internal Medicine, Cardiovascular Center, Korea University Guro Hospital, Seoul, Korea. swrha617@yahoo.co.kr
- 2Department of Internal Medicine, Gachon University Gil Hospital, Incheon, Korea.
- 3Department of Internal Medicine, Sejong General Hospital, Bucheon, Korea.
- KMID: 2224951
- DOI: http://doi.org/10.4070/kcj.2013.43.4.269
Abstract
- Aortic coarctation is a correctable hypertensive disease. For safety reasons and due to the invasiveness of surgical techniques, percutaneous interventions have become drastically more popular in recent times. In elderly patients with aortic coarctation who are at risk of an aortic wall aneurysm and rupture, covered stents are preferred but in younger patients, bare metal stenting may be sufficient for long-term safety. Herein we present a 47-year-old typical aortic coarctation patient who was successfully treated with a bare metal stent.
Keyword
Figure
-
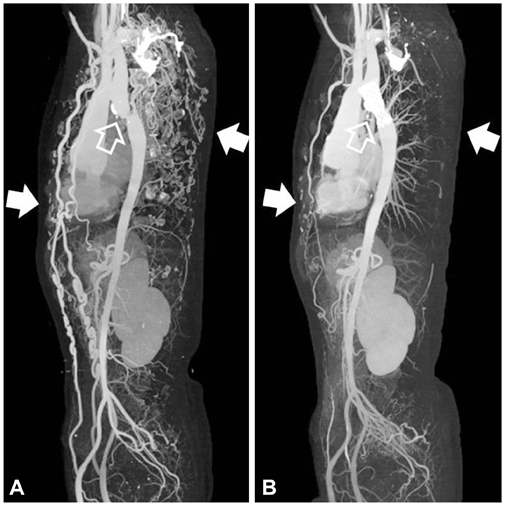
Fig. 1 Pre- and post-procedural CT angiographic findings. A: pre-procedural CT angiography showing severe coarctation of descending aorta just below the left main pulmonary artery level (transparent arrow). Note vigorous collateral blood flow of anterior and posterior trunk (white arrows). B: post-procedural CT angiography showed increased isthmus diameter from 8 to 16 mm (transparent arrow). Diminished collateral blood flow was also observed (white arrows).

Fig. 2 Invasive angiographic images of pre- and post-stenting. A: thoracic aortography showed the coarctation segment of 8 mm in diameter and 40 mm in length (arrowheads). B: successful deployment of bare metal stent using a 22×50 mm self-expandable nitinol stent showing correct device position without any immediate dissection or perforation (arrowheads).

Fig. 3 Bare metal stent, pre-mounting state. Hercules vascular stent, S&G, made out of shape memory nitinol with a semi-opencell structure and reconstrainable design. This bare metal stent, which is manufactured in Korea, is available for a diameter of 8 to 22 mm and length of 40 to 120 mm.
Reference
-
1. Keith DS, Markey B, Schiedler M. Successful long-term stenting of an atypical descending aortic coarctation. J Vasc Surg. 2002. 35:166–167.2. Mullen MJ. Coarctation of the aorta in adults: do we need surgeons? Heart. 2003. 89:3–5.3. Teixeira AM, Anjos R, Abecasis M, Cordeiro P, Ferreira R, Martins M. Stents for correction of aortic coarctation in adults. Rev Port Cardiol. 2005. 24:1559–1563.4. Butera G, Piazza L, Chessa M, et al. Covered stents in patients with complex aortic coarctations. Am Heart J. 2007. 154:795–800.5. Tzifa A, Ewert P, Brzezinska-Rajszys G, et al. Covered Cheatham-platinum stents for aortic coarctation: early and intermediate-term results. J Am Coll Cardiol. 2006. 47:1457–1463.6. Orend KH, Zarbis N, Schelzig H, Halter G, Lang G, Sunder-Plassmann L. Endovascular treatment (EVT) of acute traumatic lesions of the descending thoracic aorta--7 years' experience. Eur J Vasc Endovasc Surg. 2007. 34:666–672.7. Grech V. Diagnostic and surgical trends, and epidemiology of coarctation of the aorta in a population-based study. Int J Cardiol. 1999. 68:197–202.8. Cevik S, Izgi C, Cevik C. Asymptomatic severe aortic coarctation in an 80-year-old man. Tex Heart Inst J. 2004. 31:429–431.9. Brickner ME, Hillis LD, Lange RA. Congenital heart disease in adults. First of two parts. N Engl J Med. 2000. 342:256–263.10. Kenny D, Hijazi ZM. Coarctation of the aorta: from fetal life to adulthood. Cardiol J. 2011. 18:487–495.11. Tanous D, Benson LN, Horlick EM. Coarctation of the aorta: evaluation and management. Curr Opin Cardiol. 2009. 24:509–515.12. Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to develop guidelines on the management of adults with congenital heart disease). Circulation. 2008. 118:e714–e833.13. Carr JA. The results of catheter-based therapy compared with surgical repair of adult aortic coarctation. J Am Coll Cardiol. 2006. 47:1101–1107.14. Godart F. Intravascular stenting for the treatment of coarctation of the aorta in adolescent and adult patients. Arch Cardiovasc Dis. 2011. 104:627–635.15. Forbes TJ, Garekar S, Amin Z, et al. Procedural results and acute complications in stenting native and recurrent coarctation of the aorta in patients over 4 years of age: a multi-institutional study. Catheter Cardiovasc Interv. 2007. 70:276–285.16. Rehders TC, Petzsch M, Ince H, et al. Intentional occlusion of the left subclavian artery during stent-graft implantation in the thoracic aorta: risk and relevance. J Endovasc Ther. 2004. 11:659–666.17. Butera G, Manica JL, Chessa M, et al. Covered-stent implantation to treat aortic coarctation. Expert Rev Med Devices. 2012. 9:123–130.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Use of Covered Stents to Treat Coarctation of the Aorta
- Coarctation of the Aorta Treated with Stenting in a Patient with Turner Syndrome
- Extraanatomic Aortic Bypass through a Median Sternotomy in a Patient with Coarctation of Aorta Associated with Annuloaortic Ectasia: A case report
- A successful stenting of the coarctation of aorta in a patient with acute pulmonary edema
- Coarctation of the Aorta Associated with Chronic Thoracic Aortic Aneurysm: A case report
