A Case of Sheathless Transradial Coronary Intervention for Complex Coronary Lesions with a Standard Guiding Catheter
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Soonchunhyang University Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea. naeheelee@naver.com
- KMID: 2224934
- DOI: http://doi.org/10.4070/kcj.2013.43.5.347
Abstract
- One of the major limitations of transradial coronary intervention is the inability to use large guiding system, which leads to the development of dedicated sheathless guide catheter system. However, these devices are not available in the Republic of Korea. We present a case in which conventional guiding catheter was used for sheathless transradial coronary intervention in the treatment of complex coronary anatomy.
Keyword
Figure
-
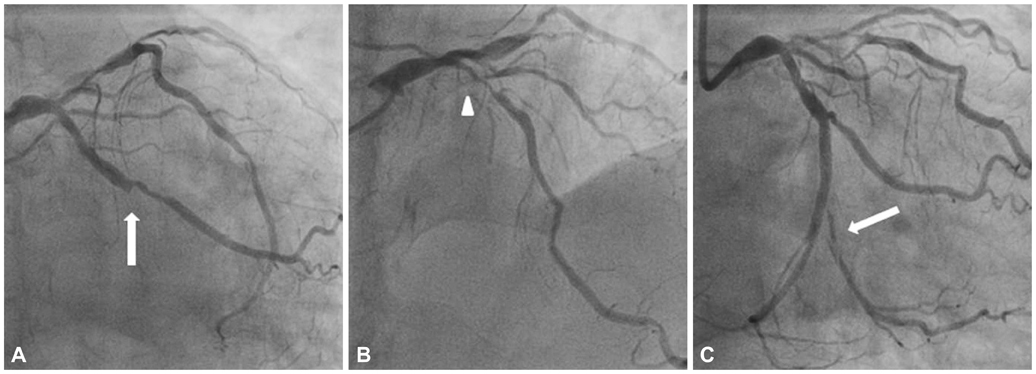
Fig. 1 The initial coronary angiography. A and B: the left coronary angiography showed total occlusion at distal left circumflex artery (arrow) and diffuse 70-90% stenosis with severe calcification at distal left main coronary artery to proximal left anteriordescending artery (arrow head). C: after implantation of stent at distal left circumflex artery, a dissection occurred at second obtuse marginal branch (arrow).
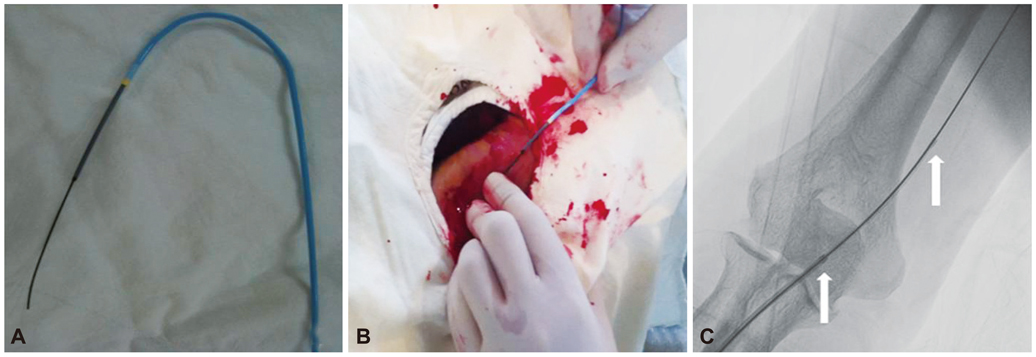
Fig. 2 Guiding catheter insertion for sheathless transradial coronary intervention. A: for easier insertion of the guiding catheter, a "pseudo-taper" was created by insertion of a 5 Fr, 120 cm Heartrail catheter into and through the 7 Fr XB 3.5 guiding catheter. B: after removal of the 5 Fr introducer sheath, both catheters were inserted through the skin into the radial artery. C: both catheters were advanced to the aortic root (arrows).
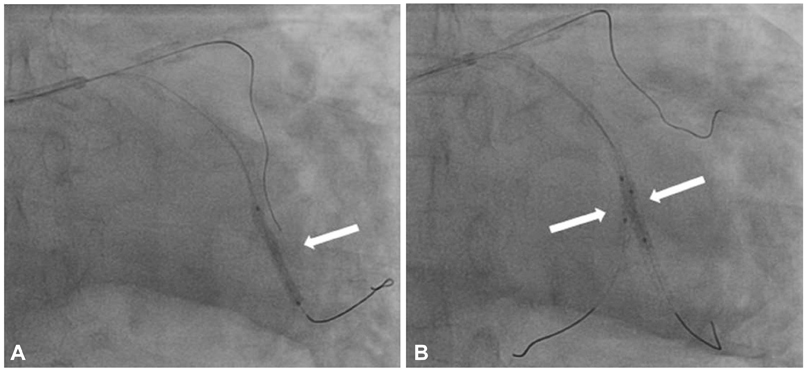
Fig. 3 The sheathless transradial coronary intervention for left circumflex lesion. A: after multiple predilatation of the second obtuse marginal branch, the stent was deployed by culottes technique across the previous left circumflex stent (arrow). B: the kissing balloon dilatation was successfully performed (arrows).
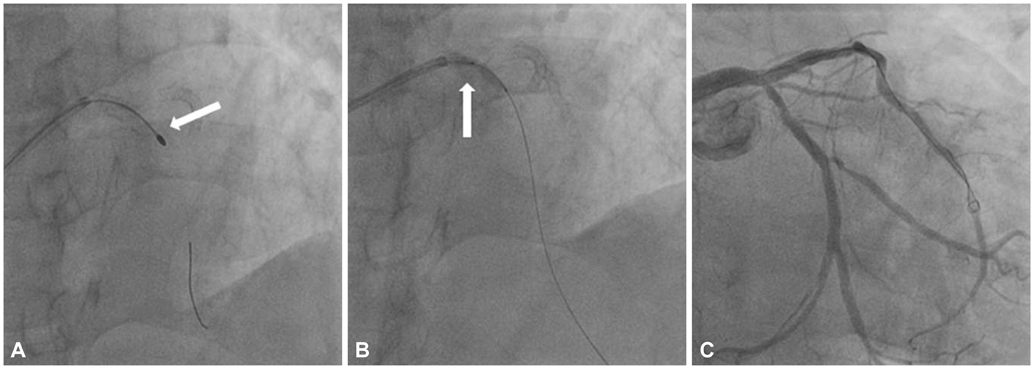
Fig. 4 The sheathless transradial coronary intervention for left anterior descending artery. A: rotational atherectomy (1.5 mm burr) was performed 5 times (arrow). B: two stents were implanted with the support of 5 Fr, 120 cm Heartrail catheter (child in mother technique) after multiple predilatations (arrow). C: the final angiography revealed excellent results.
Reference
-
1. Jolly SS, Amlani S, Hamon M, Yusuf S, Mehta SR. Radial versus femoral access for coronary angiography or intervention and the impact on major bleeding and ischemic events: a systematic review and meta-analysis of randomized trials. Am Heart J. 2009; 157:132–140.2. Agostoni P, Biondi-Zoccai GG, de Benedictis ML, et al. Radial versus femoral approach for percutaneous coronary diagnostic and interventional procedures; systematic overview and meta-analysis of randomized trials. J Am Coll Cardiol. 2004; 44:349–356.3. Saito S, Ikei H, Hosokawa G, Tanaka S. Influence of the ratio between radial artery inner diameter and sheath outer diameter on radial artery flow after transradial coronary intervention. Catheter Cardiovasc Interv. 1999; 46:173–178.4. Yoo BS, Yoon J, Ko JY, et al. Anatomical consideration of the radial artery for transradial coronary procedures: arterial diameter, branching anomaly and vessel tortuosity. Int J Cardiol. 2005; 101:421–427.5. Dahm JB, Vogelgesang D, Hummel A, Staudt A, Völzke H, Felix SB. A randomized trial of 5 vs. 6 French transradial percutaneous coronary interventions. Catheter Cardiovasc Interv. 2002; 57:172–176.6. Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T, van der Wieken R. A randomized comparison of percutaneous transluminal coronary angioplasty by the radial, brachial and femoral approaches: the access study. J Am Coll Cardiol. 1997; 29:1269–1275.7. Sakai H, Ikeda S, Harada T, et al. Limitations of successive transradial approach in the same arm: the Japanese experience. Catheter Cardiovasc Interv. 2001; 54:204–208.8. Cogliano MA, Tolerico PH. Nonhealing wound resulting from a foreign body to a radial arterial sheath and sterile inflammation associated with transradial catheterization and hydrophilic sheaths. Catheter Cardiovasc Interv. 2004; 63:104–105.9. Kozak M, Adams DR, Ioffreda MD, et al. Sterile inflammation associated with transradial catheterization and hydrophilic sheaths. Catheter Cardiovasc Interv. 2003; 59:207–213.10. Mamas MA, Fath-Ordoubadi F, Fraser DG. Atraumatic complex transradial intervention using large bore sheathless guide catheter. Catheter Cardiovasc Interv. 2008; 72:357–364.11. Liang M, Puri A, Linder R. Transradial simultaneous kissing stenting (SKS) with SheathLess access. Catheter Cardiovasc Interv. 2010; 75:222–224.12. Youn YJ, Yoon J, Han SW, et al. Feasibility of transradial coronary intervention using a sheathless guiding catheter in patients with small radial artery. Korean Circ J. 2011; 41:143–148.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful transradial intervention via a radial recurrent artery branch from the radioulnar alpha loop using a sheathless guiding catheter
- Feasibility of Transradial Coronary Intervention Using a Sheathless Guiding Catheter in Patients With Small Radial Artery
- Simple Management of Radial Artery Perforation during Transradial Percutaneous Coronary Intervention
- Removal of Dislodged Stent by Using 8 Fr Sheath and Forcep during Transradial Coronary Stenting
- Usefulness of Deep Seating Technique for Transradial Coronary Intervention
