Korean Circ J.
2013 Dec;43(12):830-833. 10.4070/kcj.2013.43.12.830.
Repeated Aborted Sudden Cardiac Death with Long QT Syndrome in a Patient with Anomalous Origin of the Right Coronary Artery from the Left Coronary Cusp
- Affiliations
-
- 1Cardiology Division, Gachon University Gil Hospital, Incheon, Korea. cis@gilhospital.com
- 2Thoracic and Cardiovascular Surgery Division, Gachon University Gil Hospital, Incheon, Korea.
- KMID: 2224778
- DOI: http://doi.org/10.4070/kcj.2013.43.12.830
Abstract
- A 15-year-old female with a prior history of aborted cardiac death and surgical correction of anomalous origin of the right coronary artery (RCA) presented with polymorphic ventricular tachycardia. Her electrocardiogram after defibrillation was suggestive of congenital long QT syndrome (LQTS). The patient was treated with a beta-blocker and remained free from ventricular arrhythmia during the follow-up of more than 6 months. Here, we present the case of a young female with repeated aborted cardiac death accompanied by anomalous origin of the RCA and congenital LQTS for the first time.
MeSH Terms
Figure
-
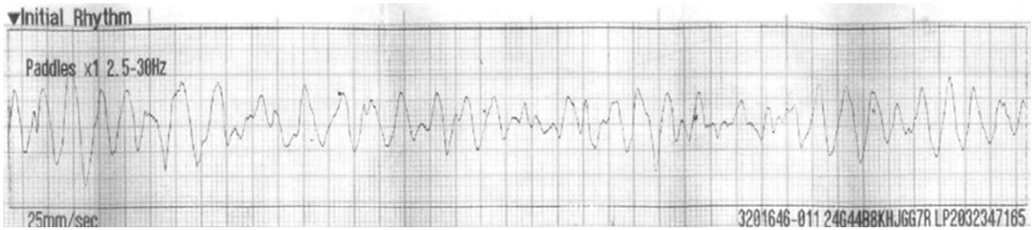
Fig. 1 A 15-year-old female was referred to the cardiology department due to repeated aborted sudden cardiac death. Initial electrocardiogram showed polymorphic ventricular tachycardia.

Fig. 2 Cardiac computed tomography revealed anomalous origin of the RCA from the left coronary cusp coursing between the pulmonary artery and the aorta (white arrows). Ao: aorta, RCA: right coronary artery, PA: pulmonary artery.
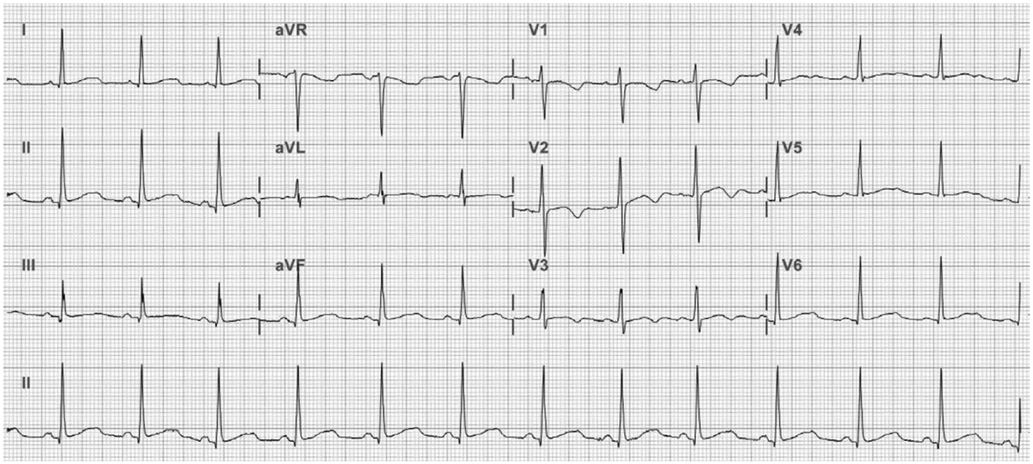
Fig. 3 Her follow-up electrocardiogram after stabilization showed a sinus rhythm with an inverted T wave and a prolonged QT interval: 470 ms, and QTc: 531 ms, which was suggestive of congenital long QT syndrome.
Reference
-
1. El-Sherif N, Chinushi M, Caref EB, Restivo M. Electrophysiological mechanism of the characteristic electrocardiographic morphology of torsade de pointes tachyarrhythmias in the long-QT syndrome: detailed analysis of ventricular tridimensional activation patterns. Circulation. 1997; 96:4392–4399.2. Tester DJ, Will ML, Haglund CM, Ackerman MJ. Effect of clinical phenotype on yield of long QT syndrome genetic testing. J Am Coll Cardiol. 2006; 47:764–768.3. Angelini P. Coronary artery anomalies--current clinical issues: definitions, classification, incidence, clinical relevance, and treatment guidelines. Tex Heart Inst J. 2002; 29:271–278.4. Shimizu W, Antzelevitch C. Sodium channel block with mexiletine is effective in reducing dispersion of repolarization and preventing torsade des pointes in LQT2 and LQT3 models of the long-QT syndrome. Circulation. 1997; 96:2038–2047.5. Kawabata M, Hirao K, Takeshi S, et al. Torsades de pointes related to transient marked QT prolongation following successful emergent percutaneous coronary intervention for acute coronary syndrome. J Electrocardiol. 2008; 41:117–122.6. Moreno FL, Villanueva T, Karagounis LA, Anderson JL. TEAM-2 Study Investigators. Reduction in QT interval dispersion by successful thrombolytic therapy in acute myocardial infarction. Circulation. 1994; 90:94–100.7. Chauhan VS, Tang AS. Dynamic changes of QT interval and QT dispersion in non-Q-wave and Q-wave myocardial infarction. J Electrocardiol. 2001; 34:109–117.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sudden Death Associated with Anomalous Left Coronary Artery Origin from Right Sinus of Valsalva with Posterior Course
- Coronary Artery Transfer for Anomalous Origin of Left Coronary Artery from Right Coronary Sinus
- A Case of Aborted Sudden Cardiac Death during Exercise Associated with an Anomalous Origin of Right Coronary Artery
- Two Cases of Anomalous Origin of Coronary Artery
- Anomalous Right Coronary Artery From the Left Coronary Sinus With an Interarterial Course: Is It Really Dangerous?
