Stroke in a Young Individual with Left Ventricular Noncompaction and Left Atrium Standstill
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Inje University College of Medicine, Busan Paik Hostpital, Busan, Korea. epkimdk@paik.ac.kr
- KMID: 2223809
- DOI: http://doi.org/10.4070/kcj.2015.45.5.432
Abstract
- Isolated left ventricular noncompaction (LVNC) is a rare cardiomyopathy with morphologic characteristics of two distinct myocardial layers i.e., thin compacted epicardial and thick noncompacted endocardial layers. The noncompacted myocardium consists of prominent ventricular trabeculae and deep intertrabecular recesses. It can lead to arrhythmias, heart failure or systemic embolisms. Electrocardiographic patterns of patients with LVNC are various and non-specific; however, the most common findings are intraventricular conduction delay, left ventricular hypertrophy, and repolarization abnormalities. We reported the first case, to the best of our knowledge, of a 29-year-old man who had recent cerebral infarction and incidental LVNC with spontaneous left atrial standstill.
MeSH Terms
Figure
-

Fig. 1 Local brain MRI showing focal high signal intensity lesions in the left temporal lobe (A. red circle) and left frontal lobe (B. yellow circle) on diffusion weighted image. MRI: magneticresonance imaging.
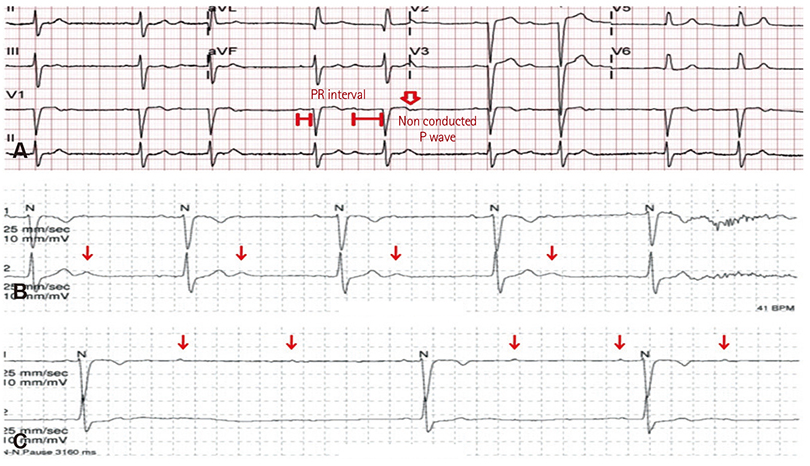
Fig. 2 (A) Electrocardiogram showing bradycardia (55 beats/min), PR prolongation followed by AV block demonstrating characteristic of second degree AV block, Mobitz type 1, left axis deviation and poor R wave progression. (B and C; red arrows mean P wave) 24 hour Holter monitoring showing intermittent 2:1 AV block with high grade AV block. AV: atrioventricular.

Fig. 3 (A) Transthoracic echocardiography (TTE). A-(a): Arrow shows heavy trabeculations in LV apex. A-(b): Due to trabeculations, myocardium of LV apex has a spongy appearance on the short axis view of TTE. (B) Contrast echocardiography. B-(a): Arrow shows heavy trabeculations in heavy trabeculations in LV apex is clearly observed with noncompacted/compacted ratio of approximately 3:1. B-(b): Arrow shows communicating flow in multiple intertrabecular recesses with LV cavity. LV: left ventricle.

Fig. 4 Cardiac MRI showing prominent trabeculations and deep intertrabecular recesses (red line) with thinner compact epicardial side (yellow line) with noncompacted/compacted ratio of approximately 3:1. MRI: magnetic resonance imaging, RV: right ventricle, LV: left ventricle.
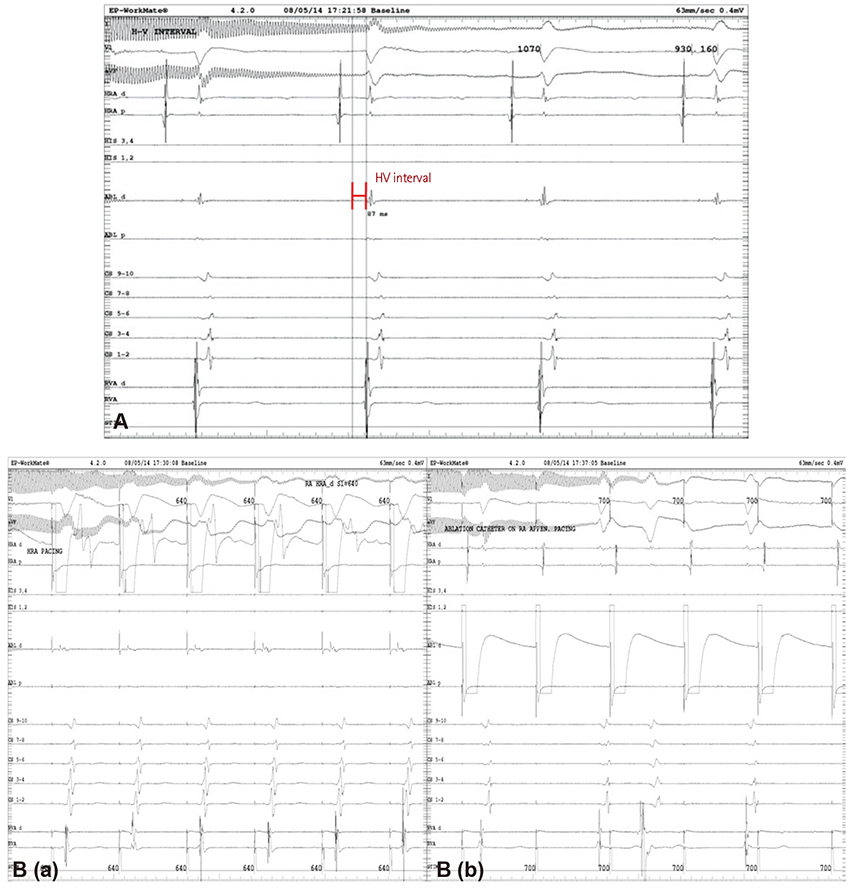
Fig. 5 Electrophysiologic test. A: Study demonstrates prolongation of HV interval of 87 msec. B-(a): Study showing 1:1 AV relationship during pacing from high RA. B-(b): Study demonstrating no atrial signal on CS bipole with no correlation between atrial and ventricular signal while pacing from RA appendage. HV: his-ventricular, AV: atrioventricular, RA: right atrium, CS: coronary sinus.

Fig. 6 3-dimensional voltage mapping. (A) Voltage signal of RA demonstrating remnant signal of RA appendage and anterior superior annulus. (B) No voltage signal was detected on LA. RA: right atrium, LA: left atrium.
Reference
-
1. Thuny F, Jacquier A, Jop B, et al. Assessment of left ventricular noncompaction in adults: side-by-side comparison of cardiac magnetic resonance imaging with echocardiography. Arch Cardiovasc Dis. 2010; 103:150–159.2. Pitta S, Thatai D, Afonso L. Thromboembolic complications of left ventricular noncompaction: case report and brief review of the literature. J Clin Ultrasound. 2007; 35:465–468.3. Weiford BC, Subbarao VD, Mulhern KM. Noncompaction of the ventricular myocardium. Circulation. 2004; 109:2965–2971.4. Dusek J, Ostádal B, Duskova M. Postnatal persistence of spongy myocardium with embryonic blood supply. Arch Pathol. 1975; 99:312–317.5. Chin TK, Perloff JK, Williams RG, Jue K, Mohrmann R. Isolated noncompaction of left ventricular myocardium. A study of eight cases. Circulation. 1990; 82:507–513.6. Habib G, Charron P, Eicher JC, et al. Isolated left ventricular noncompaction in adults: clinical and echocardiographic features in 105 patients. Results from a French registry. Eur J Heart Fail. 2011; 13:177–185.7. Jenni R, Oechslin E, Schneider J, Attenhofer Jost C, Kaufmann PA. Echocardiographic and pathoanatomical characteristics of isolated left ventricular non-compaction: a step towards classification as a distinct cardiomyopathy. Heart. 2001; 86:666–671.8. Stöllberger C, Finsterer J, Blazek G. Left ventricular hypertrabeculation/noncompaction and association with additional cardiac abnormalities and neuromuscular disorders. Am J Cardiol. 2002; 90:899–902.9. Petersen SE, Selvanayagam JB, Wiesmann F, et al. Left ventricular non-compaction: insights from cardiovascular magnetic resonance imaging. J Am Coll Cardiol. 2005; 46:101–105.10. Jacquier A, Thuny F, Jop B, et al. Measurement of trabeculated left ventricular mass using cardiac magnetic resonance imaging in the diagnosis of left ventricular non-compaction. Eur Heart J. 2010; 31:1098–1104.11. Stanton C, Bruce C, Connolly H, et al. Isolated left ventricular noncompaction syndrome. Am J Cardiol. 2009; 104:1135–1138.12. Aras D, Tufekcioglu O, Ergun K, et al. Clinical features of isolated ventricular noncompaction in adults long-term clinical course, echocardiographic properties, and predictors of left ventricular failure. J Card Fail. 2006; 12:726–733.13. Steffel J, Kobza R, Oechslin E, Jenni R, Duru F. Electrocardiographic characteristics at Initial diagnosis in patients with isolated left ventricular noncompaction. Am J Cardiol. 2009; 104:984–989.14. Groenewegen WA, Firouzi M, Bezzina CR, et al. A cardiac sodium channel mutation cosegregates with a rare connexin40 genotype in familial atrial standstill. Circ Res. 2003; 92:14–22.15. Duncan E, Schilling RJ, Earley M. Isolated left atrial standstill identified during catheter ablation. Pacing Clin Electrophysiol. 2013; 36:e120–e124.16. Fazelifar AF, Arya A, Haghjoo M, Sadr-Ameli MA. Familial atrial standstill in association with dilated cardiomyopathy. Pacing Clin Electrophysiol. 2005; 28:1005–1008.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anesthetic experience of patient with isolated left ventricular noncompaction: a case report
- Noncompaction of Ventricular Myocardium Involving the Right Ventricle
- Left Ventricular Noncompaction Associated with Hypertrophic Cardiomyopathy: Morphologic and Functional Evaluation with Multidetector CT
- Cardiac MRI and Transthoracic Echocardiography of Left Ventricular Myocardial Noncompaction in A Patient with Congestive Heart Failure: A Case Report
- A Case of Noncompaction of the Ventricular Myocardium Combined with Situs Ambiguous with Polysplenia
